Multiphasic Contrast Computerised
Tomography
•Liver has dual blood supply
• Normal parenchyma is supplied for 80% by the portal vein and only for 20%
by the hepatic artery
• All liver tumors get 100% of their blood supply from the hepatic artery
8.
• In Arterialphase
• hypervascular tumors will enhance via the hepatic artery
• normal liver parenchyma does not yet enhances (because contrast is not yet
in the portal venous system)
• Hypervascular tumors will enhance optimally at 35 sec after contrast injection
• Portal venous phase
• To detect hypovascular tumors
• Scanning is at about 75 seconds
9.
• Delayed Phase
•Begins at about 3-4 minutes after contrast injection
• Imaging is best done at 10 minutes
• Washout of contrast – HCC
• Retention of contrast – heamangioma
• Retention of contrast in fibrous tissue
• Capsule of HCC
• Central scar of FNH
10.
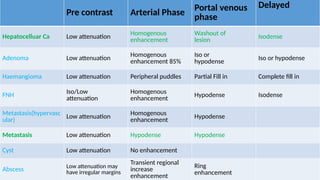
Pre contrast ArterialPhase Portal venous
phase
Delayed
Hepatocelluar Ca Low attenuation
Homogenous
enhancement
Washout of
lesion Isodense
Adenoma Low attenuation Homogenous
enhancement 85%
Iso or
hypodense
Iso or hypodense
Haemangioma Low attenuation Peripheral puddles Partial Fill in Complete fill in
FNH Iso/Low
attenuation
Homogenous
enhancement
Hypodense Isodense
Metastasis(hypervasc
ular)
Low attenuation Homogenous
enhancement
Hypodense
Metastasis Low attenuation Hypodense Hypodense
Cyst Low attenuation No enhancement
Abscess Low attenuation may
have irregular margins
Transient regional
increase
enhancement
Ring
enhancement
Liver Cell Adenoma
a relatively rare benign proliferation of hepatocytes in the
context of a normal liver
predominantly found in young women (aged 20-40 years)
associated with steroid hormone use such as oral
contraceptive pills
The female-to-male ratio is approximately 11:1
LCAs are usually singular
The presence of 10 or more adenomas is termed
adenomatosis
14.
HISTOLOGY
composed ofcords of benign hepatocytes containing
increased glycogen and fat
Bile ductules are not seen
normal architecture of the liver is not present in these
lesions
15.
CLINICAL PRESENTATION
Symptomaticin 50% to 75% of cases
MC symptom - Upper abdominal pain
tumor markers are normal
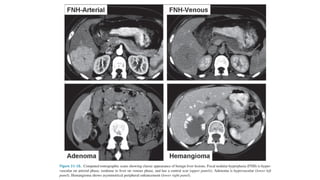
CT
a well-circumscribed heterogenous mass that shows early
enhancement during the arterial phase
MRI - pecific imaging characteristics
well-demarcated heterogenous mass containing fat or hemorrhage
resection may be necessary to secure a diagnosis in difficult
cases
16.
MANAGEMENT
acute hemorrhage- need emergent attention
hepatic artery embolization - helpful and effective temporary
maneuver
Once stabilized and appropriately resuscitated, a laparotomy and
resection of the mass is required
Symptomatic masses, likewise, are resected
Patients with asymptomatic LCA who take OCPs can be watched for
regression after stopping the OCPs
Margin status is not important in these resections, and limited
resections can be performed
17.
Focal Nodular Hyperplasia
second most common benign tumor of the liver
predominantly discovered in young women
usually a small (<5 cm) nodular mass arising in a normal
liver that involves the right and left liver equally
characterized by a central fibrous scar with radiating
septa
no central scar is seen in about 15% of cases
18.
HISTOLOGY
FNH containscords of benign-appearing hepatocytes
divided by multiple fibrous septa originating from a
central scar
Typical hepatic vascularity is not seen
atypical biliary epithelium is found scattered throughout
the lesion
The central scar often contains a large artery that
branches out into multiple smaller arteries in a spoke-
wheel pattern
19.
CLINICAL PRESENTATION
Inmost patients - incidental finding at laparotomy or more
commonly on imaging studies
most often vague abdominal pain
Physical examination is usually unrevealing
mild abnormalities of LFTs may be found
Serum AFP levels are normal
Contrast-enhanced CT and MRI have become accurate methods of
diagnosing FNH
a homogeneous mass with a central scar that rapidly enhances during the
arterial phase of contrast administration
20.
MANAGEMENT
Asymptomatic patientsmostly remain so over long periods
of time
Rupture, bleeding, and infarction are exceedingly rare
malignant degeneration of FNH has never been
reported
The treatment depends on diagnostic certainty and
symptom
21.
Asymptomatic patientswith typical radiologic features do not require
treatment
If diagnostic uncertainty exists, resection may be necessary for
histologic confirmation
Symptomatic patients are thoroughly investigated
Careful observation of symptomatic FNH with serial imaging is
reasonable because symptoms may resolve in a significant number of
cases
persistent symptomatic FNH or an enlarging mass need to be
considered for resection.
22.
Hemangioma
Hemangioma isthe most common benign tumor of the liver
occurs in women more commonly than men (3:1 ratio) and at
a mean age of about 45 years
Small capillary hemangiomas are of no clinical significance
Cavernous hemangiomas have been associated with FNH
23.
Enlargement ofhemangiomas are by ectasia rather than
neoplasia
They are usually single and less than 5 cm in diameter
occur equally in the right and left liver
greater than 5 cm are arbitrarily called giant hemangiomas.
Involution or thrombosis of hemangiomas can result in
dense fibrotic masses that may be difficult to differentiate
from malignancy
24.
CLINICAL PRESENTATION
• Mostcommonly, hemangiomas are asymptomatic and
incidentally found on imaging studies
• Large compressive masses may cause vague upper
abdominal symptoms
• Rapid expansion or acute thrombosis can, on occasion, cause
symptoms
• Spontaneous rupture is exceedingly rare
• An associated syndrome of thrombocytopenia and
consumptive coagulopathy known as Kasabach-Merritt
syndrome
25.
INVESTIGATIONS
•LFTs and tumormarkers are usually normal
•CT and MRI are usually sufficient
• typical peripheral nodular enhancement pattern
•Labeled red blood cell scans are an accurate test rarely
necessary
•Percutaneous biopsy of a suspected hemangioma is
potentially dangerous and inaccurate and is therefore not
recommended
26.
MANAGEMENT
Most ofthese tumors remain stable over long periods of time
low risk for rupture or hemorrhage
Growth and development of symptoms do occur, occasionally
requiring resection
An asymptomatic patient with a secure diagnosis can be
simply observed
Symptomatic patients are candidates for resection if no
other cause is found
27.
Rupture, changein size, and development of the Kasabach-
Merritt syndrome are indications for resection
In rare cases of diagnostic uncertainty, resection may
be necessary to make a definitive diagnosis
The preferred approach to resection is enucleation with
inflow control
28.
Liver hemangiomas inchildren
account for about 12% of all childhood hepatic tumors
usually multifocal and can involve other organs
Large hemangiomas in children can result in congestive heart failure
secondary to arteriovenous shunting
Untreated symptomatic childhood hemangiomas are associated with a 70%
mortality rate
small capillary hemangiomas almost all resolve
Symptomatic childhood hemangiomas may be treated medically for
congestive heart failure, with therapeutic embolization
Resection may be necessary for symptomatic lesions or for rupture
29.
Macroregenerative nodules
previouslyknown as adenomatous hyperplasia
single or multiple
they result from the hyperplastic response to chronic liver
injury
well-circumscribed, bile-stained, bulging surface
nodules that occur primarily in cirrhotic patients
have malignant potential
very difficult to distinguish from hepatocellular carcinoma
30.
Nodular regenerative hyperplasia(NRH)
• benign, diffuse, micronodular (usually <2 cm) process
• associated with
• lymphoproliferative disorders
• collagen vascular diseases
• use of steroids or chemotherapy
no malignant potential
not associated with cirrhosis
Biopsy may be necessary to distinguish these focal
nodules from malignancy
31.
Primary Solid MalignantNeoplasms
• Hepatocellular Carcinoma
• Most common primary malignancy of the liver
• Third most common cause of cancer related death
• The incidence of HCC is rising, largely attributed to a rise in hepatitis C
infection
32.
EPIDEMOLOGY
most commonprimary malignancy of the liver and 5th
most common malignancies worldwide
two to eight times more common in males than in females
75% to 80% of HCC cases have viral etiology
HBV (50%-55%) infection
HCV (25%-30%) infection
Cirrhosis is not required for the development of HCC
HCC is not an inevitable result of cirrhosis
33.
AETIOLOGY
Chronic alcoholabuse - increased
risk for HCC
synergistic effect with HBV and HCV
infection
Cigarette smoking - evidence is not
consistent
Congenital biliary atresia
Inborn errors of metabolism
haemochromatosis
alpha-1 antitrypsin deficiency
type 1 glycogen storage disease
Wilson disease
Chemical
Aflatoxin [Aspergillus
species]
Nitrites
Hydrocarbons &
solvents
Pesticides
Vinyl chloride
Thorotrast (colloidal
thorium dioxide)
34.
CLINICAL PRESENTATION
Mostcommonly men of 50 to 60 years of age
right upper quadrant abdominal pain and weight loss ±
palpable mass
anorexia, nausea, lethargy
hepatic decompensation in a patient with known mild cirrhosis
or even in patients without previously recognized cirrhosis
HCC can present as a rupture, hepatic vein occlusion (Budd-
Chiari syndrome), obstructive jaundice, hemobilia, or fever of
unknown origin
35.
DIAGNOSIS
• Ultrasound -significant role in screening and early
detection of HCC
• CT and MRI - definitive diagnosis and treatment planning
• An AFP level greater than 20 ng/mL is noted in about three
fourths of documented cases of HCC
• hyper vascular mass consistent with HCC combined with an
AFP higher than 400 ng/mL is diagnostic
• AFP levels are particularly useful in monitoring treated
patients for recurrence after normalization of levels
36.
Percutaneous needlebiopsies of liver lesions suspected of
being HCC are only necessary in patients who are being
considered for non-operative therapies
Contrast-enhanced CT and MRI protocols aimed at diagnosing
HCC take advantage of the hyper vascularity of these tumors,
and arterial phase images are critical to adequately assess the
extent of disease
CT and MRI also evaluate the extent of disease in terms of
peritoneal metastases, nodal metastases, and extent of
vascular and biliary involvement
37.
STAGING
A. assessing theextent of disease
Extent of disease in the liver, including macro vascular
invasion and the presence of multiple liver masses
the common sites of metastases must be considered
A preoperative chest x-ray is mandatory
Routine bone scans are not performed unless there are
suggestive symptoms or signs.
38.
B. Assessment ofliver function
absolutely critical in considering treatment options for a
patient with HCC
the risk for postoperative liver failure and death must be
considered
clinical assessment schemes most commonly, Child's status
(as modified by Pugh) is used
significant portal hypertension regardless of biochemical
assessments is highly predictive of postoperative liver
failure and death
39.
ROLE OF STAGINGLAPAROSCOPY
Staging laparoscopy has recently been employed as a
staging tool in HCC
spares about one in five patients a nontherapeutic
laparotomy
Laparoscopy yields additional information about extent of
disease in the liver, extrahepatic disease, and cirrhosis
40.
STAGING SYSTEMS
probablydepend on the specific population being staged and the
etiology of HCC in that particular population
The TNM staging system is not routinely used for HCC
does not accurately predict survival because it does not take liver
function into account
The Okuda staging system is an older but simple and effective
system that takes into account liver function and tumor-related
factors
The most well-validated staging system is the Cancer of the
Liver Italian Program (CLIP)
41.
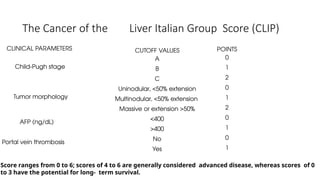
The Cancer ofthe Liver Italian Group Score (CLIP)
CLINICAL PARAMETERS
Child-Pugh stage
Tumor morphology
AFP (ng/dL)
Portal vein thrombosis
CUTOFF VALUES
A
B
C
Uninodular, <50% extension
Multinodular, <50% extension
Massive or extension >50%
<400
>400
No
Yes
Score ranges from 0 to 6; scores of 4 to 6 are generally considered advanced disease, whereas scores of 0
to 3 have the potential for long- term survival.
POINTS
0
1
2
0
1
2
0
1
0
1
42.
PATHOLOGY
Histologically, HCCis graded as well, moderately, or poorly
differentiated
The grade of HCC, however, has never been shown to
accurately predict outcome
A.HANGING TYPE
B.PUSHING TYPE
C.INFILTRTIVE TYPE
Small tumors less than 5 cm in size usually do not fall into any
of these groups and are often discussed as a separate entity
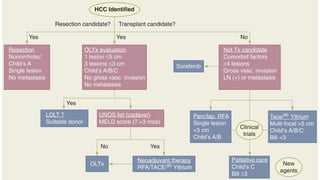
Complete excisionof HCC either by partial hepatectomy or
by total hepatectomy and transplantation is the
treatment of choice when possible because it has the
highest chance of long-term survival
only 10% to 20% of patients are considered to have
resectable disease
mortality rate less than 5% for partial hepatectomy
46.
Patients withChild's B or C cirrhosis or portal hypertension
do not tolerate resection
The volume of the future liver remnant (FLR) is also an
important consideration
Preoperative portal vein embolization is an effective
strategy to increase the volume and function of the FLR
47.
Negative Prognostic Factors
Tumour Size
Cirrhosis
Infiltrative Growth Pattern
Vascular Invasion
Intrahepatic Metastases
Multifocal Tumours
Lymph Node Metastases
Margin Less Than 1 Cm
Lack Of A Capsule
48.
ROLE OF LIVERTRANSPLANTATION
ideal treatment for HCC
addresses both the liver dysfunction and the HCC
Limitations
need for chronic immunosuppression
lack of organ donors
49.
improved outcomes
single tumors less than 5 cm
multiple tumors no more than three in number and 3 cm in size
Patients with advanced cirrhosis (Child's B and C) and
early-stage HCC are considered for transplantation
Child's A cirrhosis have similar results with transplantation
and resection and should probably undergo resection
50.
Percutaneous ethanol injection(PEI)
useful technique for ablating small tumors
The tumor is killed by a combination of cellular dehydration,
coagulative necrosis, and vascular thrombosis
tumors less than 2 cm in size can be ablated with a single
application of PEI
Larger tumors may require multiple injections
Long-term survival after PEI for tumors less than 5 cm has
been reported to range from 24% to 40
51.
Thermal ablative techniques
freeze or heat tumors to destroy them - popular in recent years
Cryotherapy
uses a specialized cryoprobe to freeze and thaw tumor and surrounding
liver tissue with resulting necrosis
usually performed at laparotomy or laparoscopically
recently been performed with percutaneous techniques
Radiofrequency ablation (RFA)
high-frequency alternating current to create heat around an inserted probe,
resulting in temperatures greater than 60°C and immediate cell death
can easily be performed percutaneously with low complication rates
52.
Transarterial therapy
Principlemost of the tumor's blood supply is by hepatic artery
Hepatic arterial infusion (HAI) chemotherapy using 5-fluorouracil
(5-FU)- based compounds, cisplatin, and doxorubicin has been
studied
requirement of a laparotomy to place the pump and associated
hepatic toxicity limits the applicability of this approach
appropriate candidates - patients with preserved liver
function and asymptomatic multinodular tumors without
vascular invasion
53.
OTHER MODALITIES
Systemicchemotherapy with a variety of agents has been
ineffective for the treatment of HCC and has a minimal
role in the treatment of HCC
External-beam radiation therapy (EBRT) has a limited role
in the treatment of HCC, although occasional dramatic
responses are seen
54.
Fibrolamellar HCC
generallyoccurs in younger patients without a history of
cirrhosis
usually well demarcated and encapsulated
may have a central fibrotic area
central scar can make distinguishing this tumor from FNH
difficult
FHCC does not produce AFP
associated with elevated neurotensin levels
55.
In general,FHCC has a better prognosis than HCC
likely related to high resectability rates, lack of chronic liver
disease, and a more indolent course
Long-term survival can be expected in about 50% to 75% of
patients after complete resection
recurrence is common and occurs in at least 80% of
patients
56.
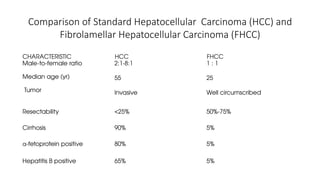
Comparison of StandardHepatocellular Carcinoma (HCC) and
Fibrolamellar Hepatocellular Carcinoma (FHCC)
CHARACTERISTIC HCC FHCC
Male-to-female ratio
Median age (yr)
Tumor
2:1-8:1
55
Invasive
1 : 1
25
Well circumscribed
Resectability <25% 50%-75%
Cirrhosis 90% 5%
α-fetoprotein positive 80% 5%
Hepatitis B positive 65% 5%
57.
Hepatic metastasis
More commonthan primary
May be solitary but usually multiple
Majority are hypovascular
Extremely variable appearance on ultrasound


![AETIOLOGY
Chronic alcohol abuse - increased
risk for HCC
synergistic effect with HBV and HCV
infection
Cigarette smoking - evidence is not
consistent
Congenital biliary atresia
Inborn errors of metabolism
haemochromatosis
alpha-1 antitrypsin deficiency
type 1 glycogen storage disease
Wilson disease
Chemical
Aflatoxin [Aspergillus
species]
Nitrites
Hydrocarbons &
solvents
Pesticides
Vinyl chloride
Thorotrast (colloidal
thorium dioxide)](https://image.slidesharecdn.com/liverneoplasms-250305151959-503f7d07/85/LIVER-NEOPLASMS-classification-example-clinical-presentation-imaging-histology-33-320.jpg)



































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)




![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)







