- This study followed women who booked home births in the UK in 1994 and matched them to similar women who booked hospital births.
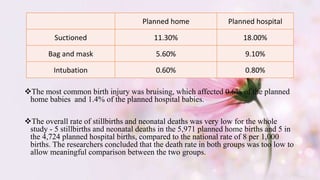
- Outcomes were recorded for 5,971 home birth women and 4,724 matched hospital birth women. The groups were low-risk and well-matched.
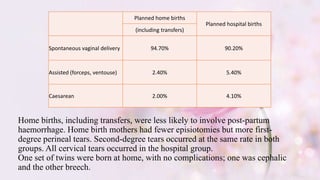
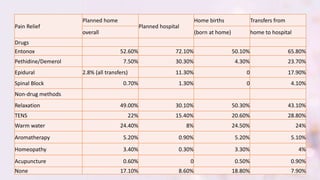
- Planning a home birth was found to halve the chances of assisted or caesarean births compared to planning a hospital birth. Home births also had less reported high blood pressure and less stressful antenatal care.
- However, bias may exist since home birth women tended to be more educated/affluent and high-risk women who transferred care were excluded.













![Class 12 1. gi 2[1]](https://cdn.slidesharecdn.com/ss_thumbnails/class12-1-gi21-130606023851-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)















































































