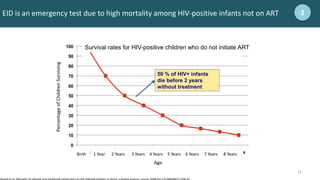
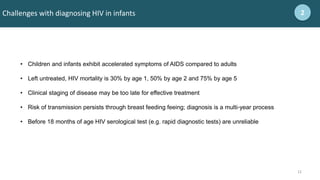
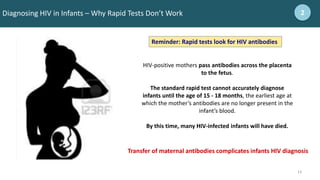
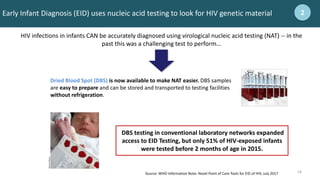
This document provides an overview of early infant diagnosis of HIV and point-of-care testing. It discusses the basics of HIV and challenges diagnosing HIV in infants. Key points include: early infant diagnosis is important due to high mortality among untreated HIV-positive infants; nucleic acid testing is used to detect HIV in infants under 18 months since antibodies may be present from the mother; and the WHO provides recommendations around testing algorithms and returning results quickly to initiate treatment if needed.

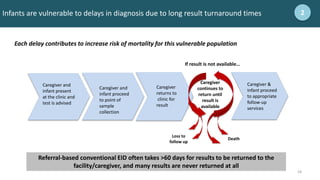
![8
8
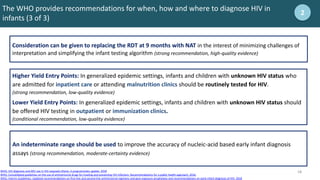
1.8 million estimated children (<15 years) living with HIV in 2017 2
Total: 1.8 million [1.3 million–2.4 million]
Middle East and North Africa
8200
[6000–11 000]
Western and central Africa
500 000
[320 000–690 000]
Eastern Europe
and central Asia
…*
Asia and the Pacific
110 000
[82 000–150 000]
North America and western and central Europe
…*
Eastern and southern Africa
1.2 million
[880 000–1.4 million]
Latin America
27 000
[19 000–36 000]
Caribbean
9900
[7400–15 000]
*Estimates for children are not published because of small numbers.
Source: UNAIDS, 2018](https://image.slidesharecdn.com/m01introductiontoeidandpoceidtesting-231117183253-28adc028/85/M01-Introduction-to-EID-and-POC-EID-Testing-pptx-8-320.jpg)
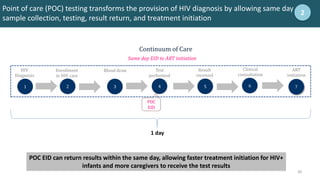
![9
9
180,000 estimated new HIV infections among children (<15 years) in 2017 2
Source: UNAIDS, 2018
Total: 180 000 [110 000–260 000]
Middle East and North Africa
1300
[780–1900]
Western and central Africa
67 000
[36 000–100 000]
Eastern Europe
and central Asia
…*
Asia and the Pacific
10 000
[7400–14 000]
North America and western and central Europe
…*
Eastern and southern Africa
92 000
[61 000–130 000]
Latin America
2400
[1800–3600]
Caribbean
1100
[710 – 1900]
*Estimates for children are not published because of small numbers.](https://image.slidesharecdn.com/m01introductiontoeidandpoceidtesting-231117183253-28adc028/85/M01-Introduction-to-EID-and-POC-EID-Testing-pptx-9-320.jpg)
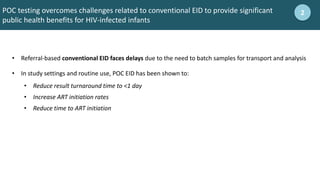
![10
10
110,00 estimated deaths in children (<15 years) from AIDS in 2017 2
Source: UNAIDS, 2018
Total: 110 000 [63 000–160 000]
Middle East and North Africa
800
[500–1200]
Western and central Africa
45 000
[24 000–69 000]
Eastern Europe
and central Asia
…*
Asia and the Pacific
6400
[4100–10 000]
North America and western and central Europe
…*
Eastern and southern Africa
52 000
[31 000–78 000]
Latin America
1700
[1200–2600]
Caribbean
700
[<500 – 1300]
*Estimates for children are not published because of small numbers.](https://image.slidesharecdn.com/m01introductiontoeidandpoceidtesting-231117183253-28adc028/85/M01-Introduction-to-EID-and-POC-EID-Testing-pptx-10-320.jpg)
![22
22
Health workers should proactively identify HIV-exposed and infected infants outside of
PMTCT
2
HIV exposed infants may present at any entry point to the facility:
• Mother-baby care point
• PMTCT
• Nutrition ward
• Young Child Clinic / Under-5 clinic
• Pediatric inpatient clinic
• TB Clinic
• Immunization / EPI
• Outpatient department
[Before the training begins, update this slide with the appropriate names of entry points in the local health system
– the names for these clinics may vary by country, but should include any ward where infants may present for care]](https://image.slidesharecdn.com/m01introductiontoeidandpoceidtesting-231117183253-28adc028/85/M01-Introduction-to-EID-and-POC-EID-Testing-pptx-22-320.jpg)
![25
25
National EID clinical algorithm 3
[Before conducting training, insert country-specific EID testing algorithm here.
During training, carefully review the algorithm, including the infant’s age when
each test should be conducted and the type of test that should be conducted.
Emphasis should be given to completing the entire EID algorithm through the
end of the exposure period (3-months after cessation of breastfeeding)]](https://image.slidesharecdn.com/m01introductiontoeidandpoceidtesting-231117183253-28adc028/85/M01-Introduction-to-EID-and-POC-EID-Testing-pptx-25-320.jpg)
![Example: POC EID Testing SOPs
ELIGIBILITY
Based on the EID national testing algorithm for molecular testing (EID NAT)
TRIAGE*
If there are more than four clients, triage based on the following criteria:
• Sick children – the sicker children given testing priority
• Distance to the facility – those having to travel furthest given testing priority
• Willingness of the caregiver to stay around for the test and results – personal judgement of
the end user, taking in to consideration the other clients in queue
POC EID TEST RESULTS
1. HIV-1 detected, perform a confirmatory test using a new sample
• If detected return results to client, and manage the client according to National HIV
Guidelines.
• If NOT detected on repeat test, collect DBS and send to molecular lab for test rerun; retain
the infant/child on preventive therapy until DBS results are out.
2. HIV-1 undetected, manage client according to National HIV Guidelines.
*Validate during clinical system training session
3
[Before conducting training, update this slide with an example that aligns with local EID SOPs]](https://image.slidesharecdn.com/m01introductiontoeidandpoceidtesting-231117183253-28adc028/85/M01-Introduction-to-EID-and-POC-EID-Testing-pptx-26-320.jpg)