Downloaded 169 times

![VIRUSES
1]Infecting CNS-Japanese encephalitis
2]Infecting RESPIRATORY SYSTEM
-SARS
-Pandemic influenza](https://image.slidesharecdn.com/viralemergingandre-emergingdiseases-150513042055-lva1-app6892/85/Viral-emerging-and-re-emerging-diseases-2-320.jpg)

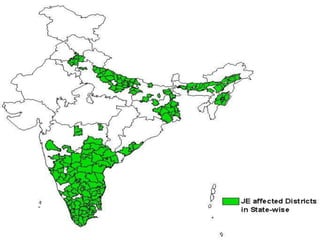
![ 1940 to 1978
› Disease spread with epidemics in China,
Korea, and India [Tamilnadu-1955]](https://image.slidesharecdn.com/viralemergingandre-emergingdiseases-150513042055-lva1-app6892/85/Viral-emerging-and-re-emerging-diseases-5-320.jpg)
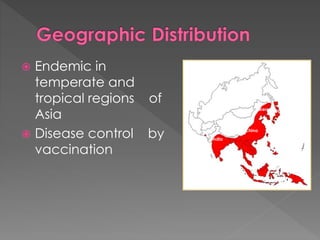






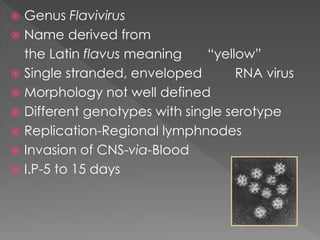
The document discusses various viruses affecting the central nervous system and respiratory system, focusing on Japanese Encephalitis (JE), SARS, and seasonal influenza. It outlines the transmission, clinical features, diagnosis, treatment, and prevention of these diseases, with emphasis on vaccination and vector control for JE. Additionally, it highlights the historical impact of influenza pandemics and the need for rapid response and international collaboration during outbreaks.




















































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)










