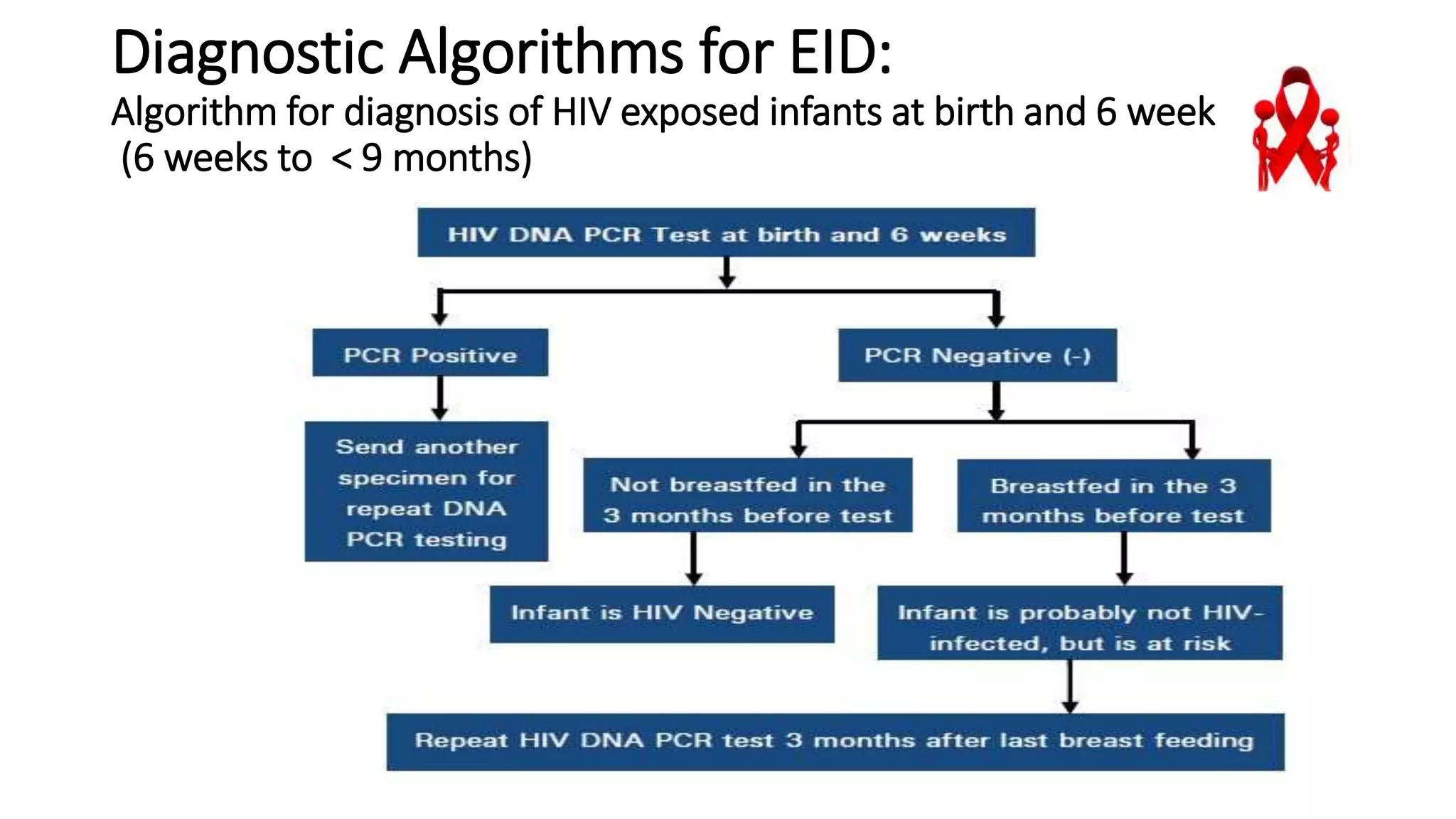
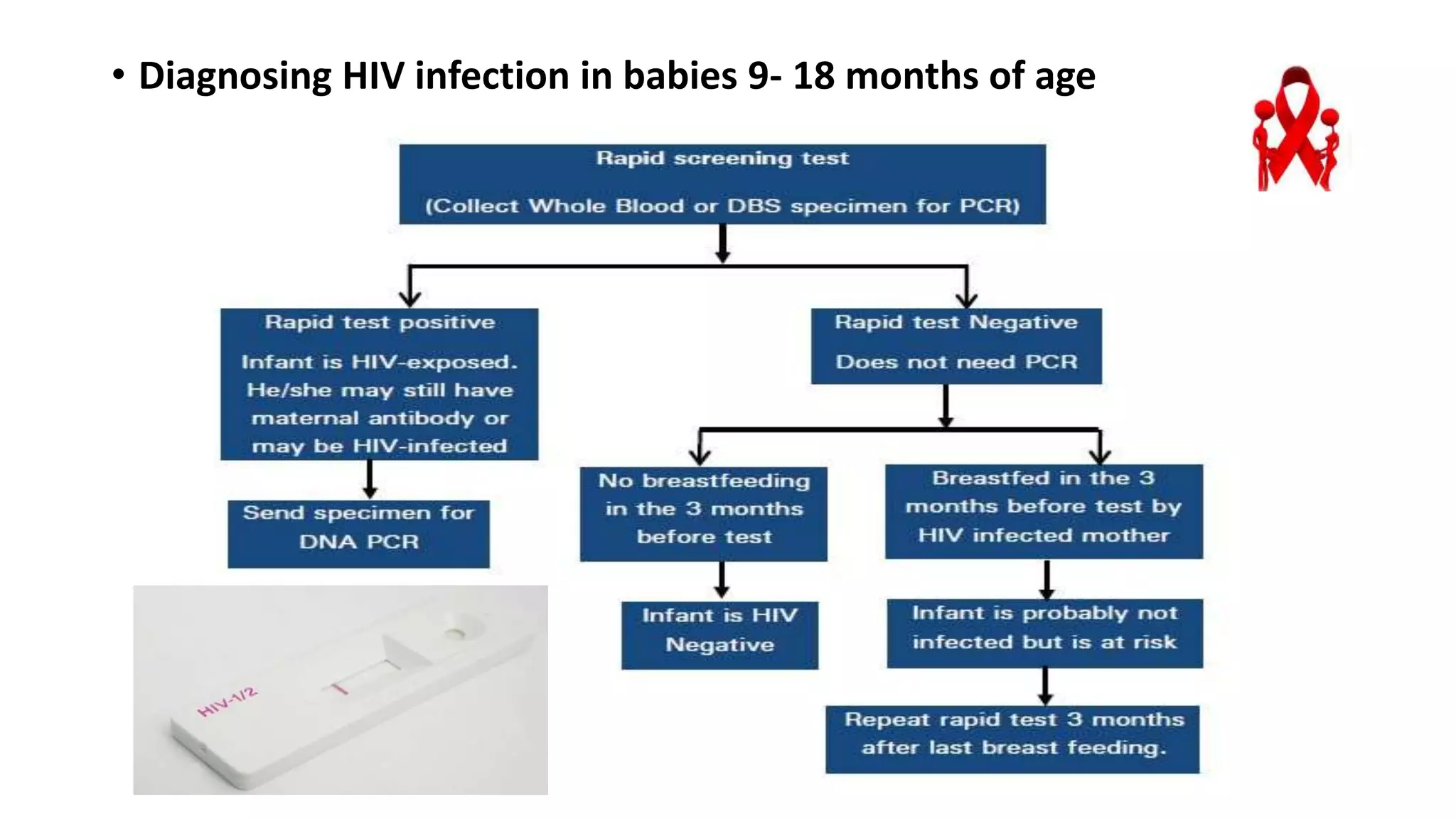
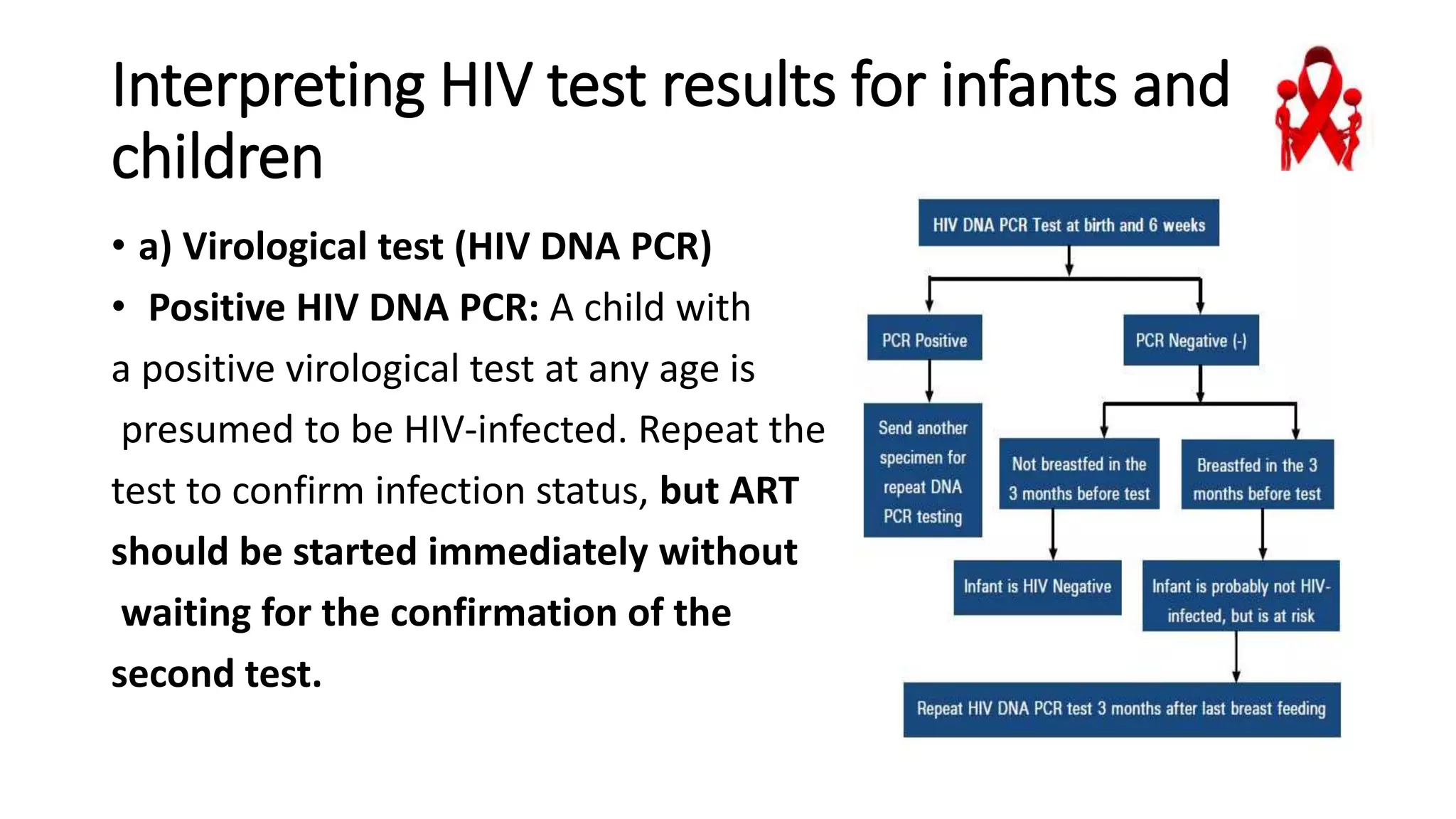
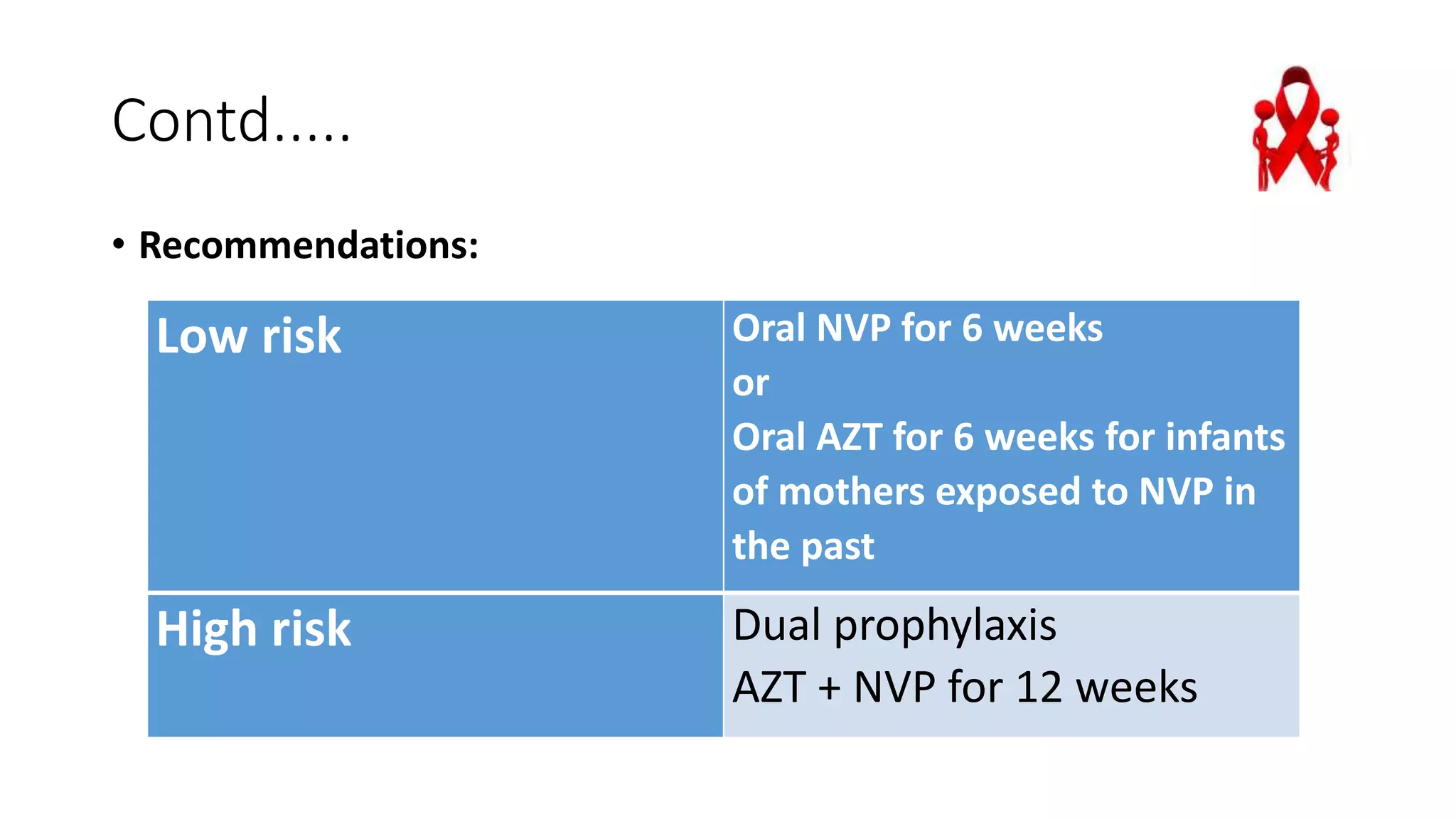
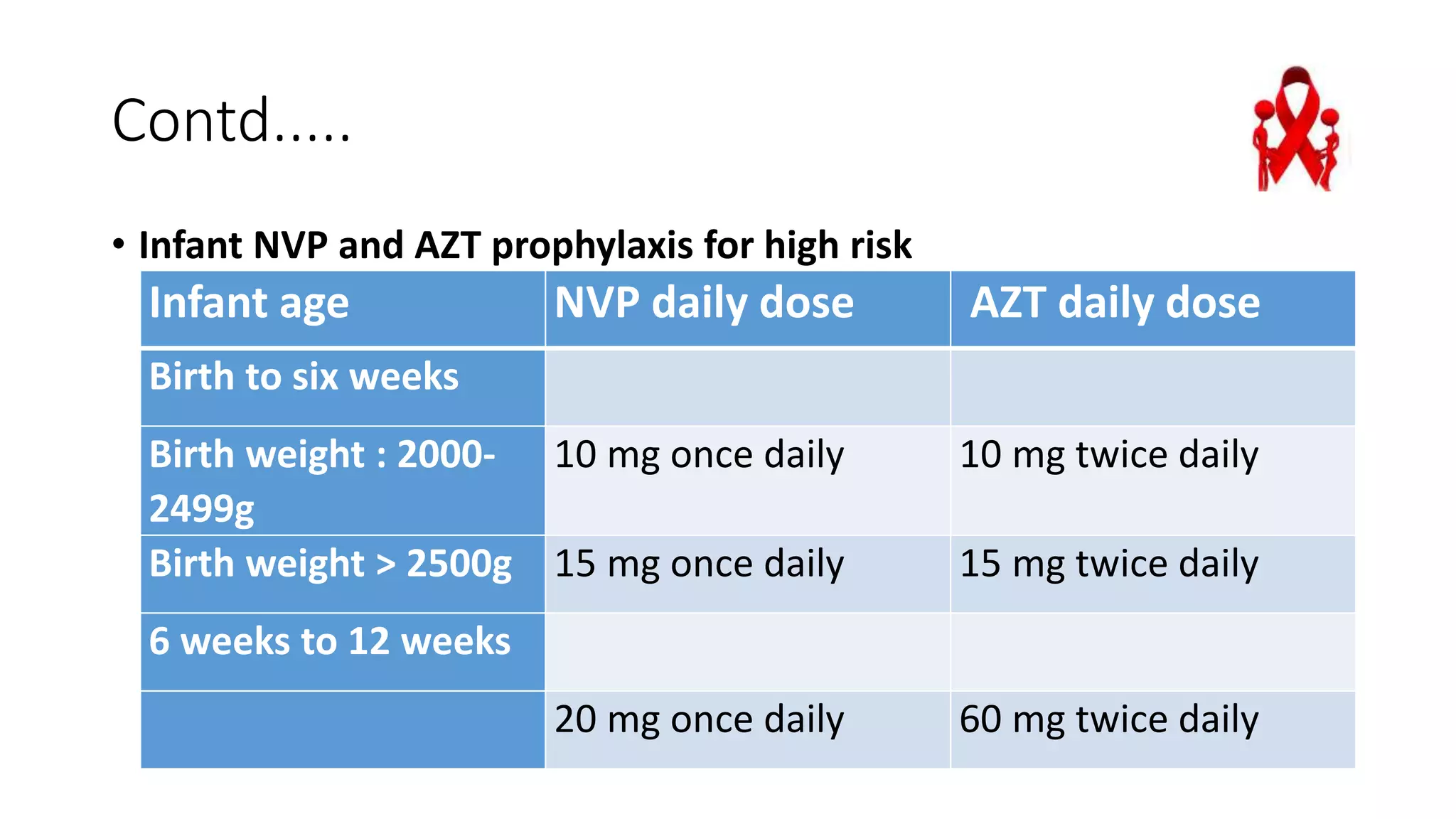
This document discusses post exposure prophylaxis with antiretroviral (ARV) drugs for HIV exposed infants. It recommends that all HIV exposed infants receive ARV prophylaxis as soon as possible after birth to reduce HIV transmission risk. For low risk infants, oral nevirapine is recommended for 6 weeks. For high risk infants, dual prophylaxis with oral zidovudine and nevirapine is recommended for 12 weeks. Polymerase chain reaction testing is used to diagnose HIV infection in infants under 18 months since antibodies can be passively transferred from the mother.