
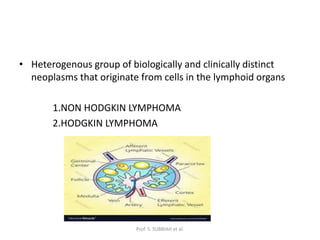


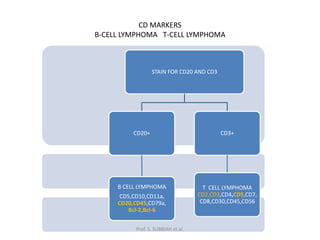





























This document discusses lymphoma, including Hodgkin and non-Hodgkin lymphoma. It provides information on the classification, staging, diagnostic testing, prognostic factors, and treatment approaches for both diseases. Key points include that lymphoma originates from lymphoid cells, the Reed-Sternberg cell is characteristic of Hodgkin lymphoma, staging involves the Ann Arbor system, and treatment often involves chemotherapy such as ABVD or R-CHOP depending on the specific lymphoma subtype and stage.























































































