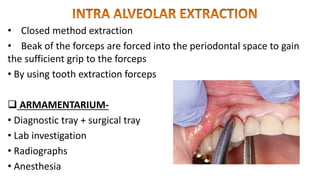
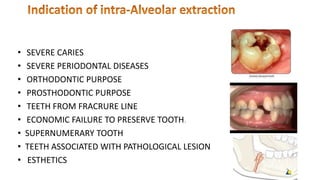
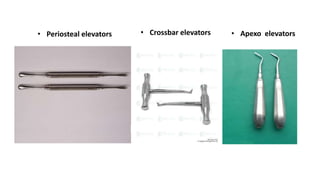
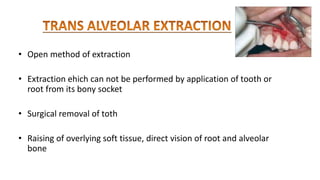
This document provides an overview of exodontia (tooth extraction). It defines exodontia and ideal tooth extraction. It discusses types of extraction including closed and open extractions. It outlines indications, contraindications, instruments used, and complications of extraction. Post-extraction care is also summarized, including inspection of the socket, medication, and follow-up care.