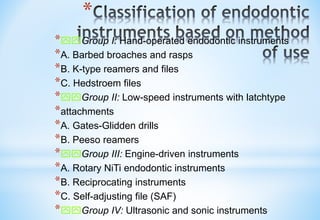
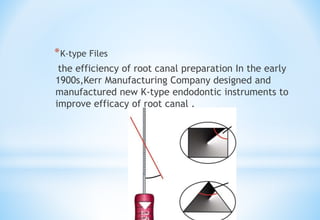
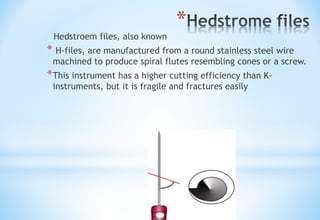
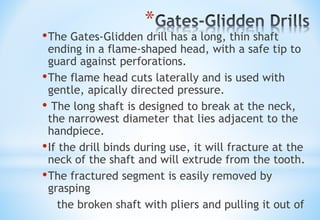
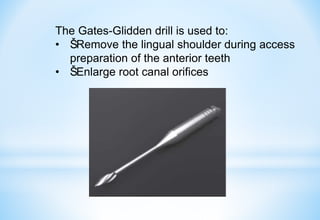
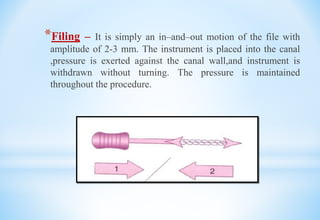
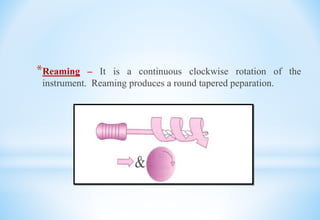
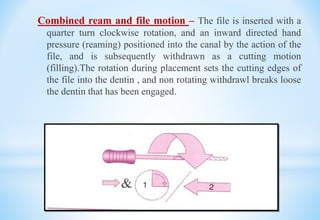
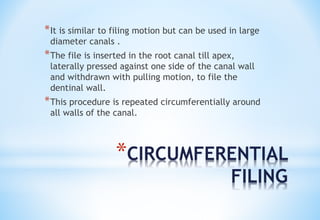
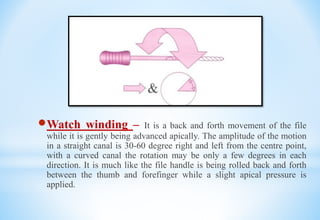
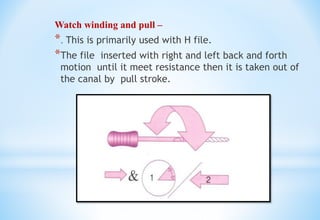
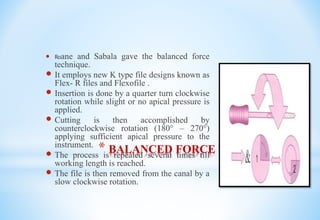
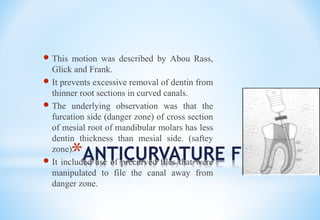
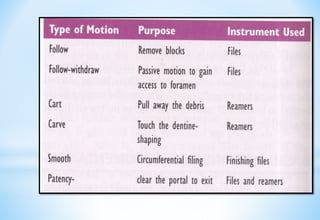
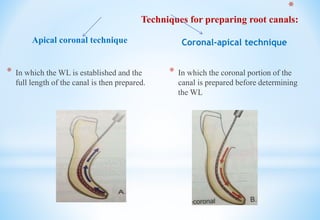
This document discusses preparation of the radicular space, including definitions, classification, objectives, and techniques for cleaning and shaping the root canal. It describes various instruments used historically and currently, including hand files, reamers, drills, and engine-driven instruments. Motions for cleaning and shaping are filing, reaming, watch winding, and balanced force. Techniques include apical-coronal and coronal-apical preparation. The goals are to remove debris, maintain canal shape, and allow filling.