Lower extremity grays
•Download as PPT, PDF•
0 likes•93 views

This document provides an overview of the anatomy of the lower limb. It describes the bones, joints, muscles, nerves, blood vessels, and surface landmarks. The key bones discussed are the femur, tibia, fibula, patella, tarsals, metatarsals, and phalanges. Major joints include the hip, knee, ankle. Muscle groups are organized by location such as gluteal, thigh, leg compartments. The lumbar and sacral plexuses and their branches are outlined. Arterial supply originates from the common iliac artery.

More Related Content
What's hot
What's hot (20)
Similar to Lower extremity grays
Similar to Lower extremity grays (20)
More from Emad Abu Alrub
Recently uploaded
Recently uploaded (20)
Lower extremity grays
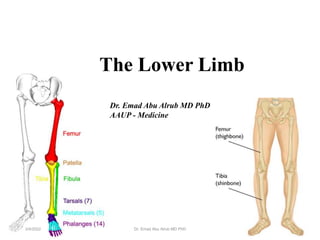
- 1. The Lower Limb 1 Dr. Emad Abu Alrub MD PhD AAUP - Medicine 3/4/2022 Dr. Emad Abu Alrub MD PhD
- 2. Surface Anatomy • Gluteal region / posterior pelvis • Iliac crest • Gluteus maximus • Cheeks • Natal/gluteal cleft • Vertical midline; “Crack” • Gluteal folds • Bottom of cheek; “prominence” 2 3/4/2022 Dr. Emad Abu Alrub MD PhD
- 3. Surface Anatomy • Anterior thigh and leg • Palpate • Patella • Condyles of femur • Femoral Triangle • Boundaries: • Sartorius (lateral) • Adductor longus (medial) • Inguinal ligament (superior) • Contents: • Femoral artery, vein and nerve, lymph nodes 3 3/4/2022 Dr. Emad Abu Alrub MD PhD
- 4. Surface Anatomy • Posterior leg • Popliteal fossa • Diamond-shape fossa behind knee • Boundaries • Biceps femoris (superior-lateral) • Semitendinosis and semimembranosis (superior- medial) • Gastrocnemius heads (inferior) • Contents • Popliteal artery and vein • Calcaneal (Achilles) tendon 4 3/4/2022 Dr. Emad Abu Alrub MD PhD
- 5. • Function: • Carry weight of entire erect body • Support • Locomotion • Points for muscular attachments • Components: • Thigh • Femur • Knee • Patella • Leg • Tibia (medial) • Fibula (lateral) • Foot • Tarsals (7) • Metatarsals (5) • Phalanges (14) Osteology/ Bones of the Lower Limb 5 3/4/2022 Dr. Emad Abu Alrub MD PhD
- 6. Acetabulum Hip joint 6 3/4/2022 Dr. Emad Abu Alrub MD PhD
- 7. Thigh • Femur • Largest, longest, strongest bone in the body!! • Receives a lot of stress • Courses medially • More in women! • Articulates with acetabulum proximally • Articulates with tibia and patella distally 7 3/4/2022 Dr. Emad Abu Alrub MD PhD
- 8. Patella • Triangular sesamoid bone • Protects knee joint • Improves leverage of thigh muscles acting across the knee 8 3/4/2022 Dr. Emad Abu Alrub MD PhD
- 9. Leg bones • Tibia • Receives the weight of body from femur and transmits to foot • Second to femur in size and weight • Articulates with fibula proximally and distally • Interosseous membrane • Fibula • Does NOT bear weight • Muscle attachment • Not part of knee joint • Stabilize ankle joint 9 3/4/2022 Dr. Emad Abu Alrub MD PhD
- 10. • Anterior leg bones • Tibia • Tibial tuberosity • Anterior crest • Medial surface • Medial malleolus • Fibula • Lateral malleolus Osteology/ Bones of the Lower Limb 10 3/4/2022 Dr. Emad Abu Alrub MD PhD
- 11. Foot • Function: • Supports the weight of the body • Act as a lever to propel the body forward • Parts: • Tarsals • Talus = ankle • Between tibia and fibula • Articulates with both • Calcaneus = heel • Attachment for Calcaneal tendon • Carries talus • Metatarsals • Phalanges 11 3/4/2022 Dr. Emad Abu Alrub MD PhD
- 12. Foot • 3 arches • Medial • Lateral • Transverse • Has tendons that run inferior to foot bones • Help support arches of foot Longitudinal 12 3/4/2022 Dr. Emad Abu Alrub MD PhD
- 13. Joints of Lower Limb • Hip (femur + acetabulum) • Ball + socket • Multiaxial • Synovial • Knee (femur + tibia) • Hinge (modified) • Biaxial • Synovial • Contains menisci, bursa, many ligaments • Knee (femur + patella) • Plane • Gliding of patella • Synovial 13 3/4/2022 Dr. Emad Abu Alrub MD PhD
- 14. Joints of Lower Limb • Proximal Tibia + Fibula • Plane, Gliding • Synovial • Distal Tibia + Fibula • Slight “give” (synarthrosis) • Fibrous (syndesmosis) • Ankle (Tibia/Fibula + Talus) • Hinge, Uniaxial • Synovial • Intertarsal & Tarsal- metatarsal • Plane, synovial • Metatarsal-phalanges • Condyloid, synovial • Interphalangeal • Hinge, uniaxial 14 3/4/2022 Dr. Emad Abu Alrub MD PhD
- 15. 15 3/4/2022 Dr. Emad Abu Alrub MD PhD
- 16. 16 3/4/2022 Dr. Emad Abu Alrub MD PhD
- 17. Muscles of Hip and Thigh • Gluteus • Posterior pelvis • Extend thigh • Rotate thigh • Abducts thigh • Anterior Compartment Thigh • Flexes thigh at hip • Extends leg at knee 17 3/4/2022 Dr. Emad Abu Alrub MD PhD
- 18. • Medial/Adductor Compartment of the thigh • Adducts thigh • Medially rotates thigh • Posterior Compartment Thigh • Extends thigh • Flexes leg 18 3/4/2022 Dr. Emad Abu Alrub MD PhD
- 19. • Gluteus maximus • Origin - Ilium, sacrum and coccyx • Insertion - Gluteal tuberosity of femur, iliotibial tract • Action - Extends thigh, lateral rotation & abduction • Innervation - Inferior gluteal nerve • Gluteus medius & Gluteus minimus • Origin – posterior Ilium • Insertion - Greater trochanter of femur • Action - Abduction, medial rotation • Innervation - Superior gluteal nerve • Lesser Gluteals help stabilize hip to allow fluent bipedal walking • Tensor fasciae latae • Origin – iliac crest and ASIS • Insertion – iliotibial tract • Action - Flex thigh, abduct thigh, medial rotation of thigh • Innervation – Superior gluteal nerve Gluteals 19 3/4/2022 Dr. Emad Abu Alrub MD PhD
- 20. Anterior Compartment Thigh • Quadriceps femoris • Rectus femoris • Origin – anterior inferior iliac spine, margin of acetabulum • Insertion – patella and tibial tuberosity via the patellar ligament • Action – extends knee, flexes thigh • Vastus lateralis • Origin-lateral proximal femur, linea aspera • Vastus medialis • Origin-medial proximal femur, linea aspera • Vastus intermedius • Origin – ant & lateral femur • Insertion for all– patella and tibial tuberosity via the patellar ligament • Action – extends knee All above innervated by the femoral nerve!!! 20 3/4/2022 Dr. Emad Abu Alrub MD PhD
- 21. Anterior Compartment Thigh • Sartorius • Origin - anterior superior iliac spine • Insertion – medial tibia • Action - flex, abduct, lat rotate thigh; weak knee flexor • Iliopsoas • Origin - Ilia, sacrum, lumbar vertebrae • Insertion – lesser trochanter of femur • Action – flexor of thigh • Innervation – femoral nerve 21 3/4/2022 Dr. Emad Abu Alrub MD PhD
- 22. Adductors • Adductor longus • Adductor brevis • Adductor magnus • Origin – inferior pelvis • Insertion – linea aspera of femur • Action – adducts and medial rotates • Innervation – Obturator nerve • Pectineus • Origin – pectineal line of pubis • Insertion – lesser trochanter of femur • Action – adducts, medial rotates • Innervation – femoral, sometimes obturator • Gracilis • Origin – inferior pubic ramus • Insertion – medial tibia • Action – adducts thigh, flex, medial, rotates leg • Innervation – Obturator nerve 22 3/4/2022 Dr. Emad Abu Alrub MD PhD
- 23. Posterior Compartment - Hamstring • Biceps femoris (2 heads) • Origin – ischial tuberosity (long) linea aspera of femur (short) • Insertion - lateral tibia, head fibula • Action - thigh extension, knee flexion, lateral rotation • Semitendinosus • Semimembranosus • Origin - ischial tuberosity • Insertion –proximal, medial tibia • Action - thigh extension, knee flexion, medial rotation Sciatic nerve innervates all of the above muscles!!! 23 3/4/2022 Dr. Emad Abu Alrub MD PhD
- 24. Muscles of the Leg • Anterior Compartment • Dorsiflex ankle, invert foot, extend toes • Innervation: Deep fibular nerve • Lateral Compartment • Plantarflex, evert foot • Innervation: Superficial Fibular nerve • Posterior Compartment • Superficial and deep layers • Plantarflex foot, flex toes • Innervation: Tibial nerve 24 3/4/2022 Dr. Emad Abu Alrub MD PhD
- 25. Anterior Compartment • Tibialis anterior • Origin - tibia • Insertion - tarsals • Action - dorsiflexion, foot inversion • Extensor digitorum longus • Origin – tibia and fibula • Insertion - phalanges • Action – toe extension • Extensor hallucis longus • Origin – fibula, interosseous membrane • Insertion – big toe • Action - extend big toe, dorsiflex foot All innervated by deep fibular nerve 25 3/4/2022 Dr. Emad Abu Alrub MD PhD
- 26. Lateral Compartment • Fibularis (peroneus) longus • Origin – lateral fibula • Insertion – 5th metatarsal, tarsal • Action - plantarflex, evert foot • Fibularis (peroneus) brevis • Origin – distal fibula • Insertion - proximal fifth metatarsal • Action – same as above!! All innervated by the superficial fibular nerve 26 3/4/2022 Dr. Emad Abu Alrub MD PhD
- 27. Superficial Posterior Compartment • Triceps surae • Gastrocnemius (2 heads) • Origin - medial and lateral condyles of femur • Insertion - posterior calcaneus via calcaneal tendon • Soleus • Origin – tibia and fibula • Insertion – same as above • Action of both – plantarflex foot • Plantaris • Origin – posterior femur • Insertion – same as above! • Action – plantarflex foot, week knee flexion All innervated by the tibial nerve 27 3/4/2022 Dr. Emad Abu Alrub MD PhD
- 28. Deep Posterior Compartment • Popliteus • Origin - lateral condyle femur and lateral meniscus • Insertion – proximal tibia • Action – flex and medially rotate leg • Flexor digitorum longus • Origin - tibia • Insertion - distal phalanges of toe 2-5 • Action – plantarflex and invert foot, flex toe • Flexor hallucis longus • Origin - fibula • Insertion - distal phalanx of hallux • Action - plantarflex and invert foot, flex toe • Tibialis posterior • Origin – tibia, fibula, and interosseous membrane • Insertion - tarsals and metatarsals • Action - plantarflex and invert foot All innervated by the tibial nerve 28 3/4/2022 Dr. Emad Abu Alrub MD PhD
- 29. Muscles of the Foot •Dorsum of Foot • Extensor digitorum brevis • O: calcaneus, I: prox phalanx of hallux • Action: extend MT-P joint • Innervation = Deep Peroneal (Fibular) n. •Plantar Surface of Foot (= sole): 4 layers • O: Tarsals and/or Metatarsals, I: Phalanges • Action: Flex, Ext, ABduct, ADduct • Innervation: Medial + Lateral Plantar n. (from Tibial n.) 29 3/4/2022 Dr. Emad Abu Alrub MD PhD
- 30. Plexuses of the Lower Limb • “Lumbosacral plexus” • Lumbar Plexus • Arises from L1-L4 • Lies within the psoas major muscle • Sacral Plexus • Arises from spinal nerve L4-S4 • Lies caudal to the lumbar plexus 30 3/4/2022 Dr. Emad Abu Alrub MD PhD
- 31. 31 3/4/2022 Dr. Emad Abu Alrub MD PhD
- 32. Lumbar Plexus • Femoral nerve • Cutaneous branches • Thigh, leg, foot (e.g. saphenous nerve) • Motor branches • Anterior thigh muscles (e.g. quadriceps, sartorius, iliopsoas) • Obturator nerve • Sensory • Skin medial thigh; hip, knee joints • Motor • Adductor muscles • Lateral femoral cutaneous • Sensory • Skin lateral thigh • Genitofemoral • Sensory • Skin scrotum, labia major, anterior thigh • Motor • Cremaster muscle 32 3/4/2022 Dr. Emad Abu Alrub MD PhD
- 33. Sacral Plexus • Sciatic • Motor: • Hamstring • Branches into: • Tibial nerve • Cutaneous • Posterior leg and sole of foot • Motor • Posterior leg, foot • Common fibular (peroneal) nerve • Cutaneous • Anterior and lateral leg, dorsum foot • Motor • Lateral compartment, tibialis anterior, toe extensors • Superior gluteal nerve • Motor • Gluteus medius and minimus, tensor fasciae latae 33 3/4/2022 Dr. Emad Abu Alrub MD PhD
- 34. Sacral Plexus • Inferior gluteal nerve • Motor • Gluteus maximus • Posterior femoral cutaneous nerve • Sensory • Inferior buttocks, posterior thigh, popliteal fossa • Pudendal nerve • Sensory • External genitalia, anus • Motor • Muscles of perineum 34 3/4/2022 Dr. Emad Abu Alrub MD PhD
- 35. 35 3/4/2022 Dr. Emad Abu Alrub MD PhD
- 36. Arteries • Common iliac (from aorta) branches into: • Internal iliac • Supplies pelvic organs • External iliac • Supplies lower limb 36 3/4/2022 Dr. Emad Abu Alrub MD PhD
- 37. Arteries • Internal iliac branches into: • Cranial and Caudal Gluteals (Superior and Inferior) • Gluteals • Internal Pudendal • Perineum, external genitalia • Obturator • Adductor muscles • Other branches supply rectum, bladder, uterus, vagina, male reproductive glands 37 3/4/2022 Dr. Emad Abu Alrub MD PhD
- 38. 38 3/4/2022 Dr. Emad Abu Alrub MD PhD
- 39. Arteries • External iliac becomes……. • Femoral • Once passes the inguinal ligament • Lower limb • Branches into Deep femoral • Adductors, hamstrings, quadriceps • Branches into Medial/lateral femoral circumflex • Head and neck of femur • Femoral becomes…… • Popliteal (continuation of femoral) • Branches into: • Geniculars • Knee • Splits into: • Anterior Tibial • Anterior leg muscles, further branches to feet • Posterior Tibial • Flexor muscles, plantar arch, branches to toes 39 3/4/2022 Dr. Emad Abu Alrub MD PhD
- 40. Veins • Deep Veins: Mostly share names of arteries • Ultimately empty into Inferior Vena Cava • Plantar • Tibial • Fibular • Popliteal • Femoral • External/internal iliac • Common iliac • Superficial Veins • Dorsal venous arch (foot) • Great saphenous (empties into femoral) • Small saphenous (empties into popliteal) 40 3/4/2022 Dr. Emad Abu Alrub MD PhD
- 41. 41 3/4/2022 Dr. Emad Abu Alrub MD PhD
- 42. DVT : Deep Venous Thrombosis 42 3/4/2022 Dr. Emad Abu Alrub MD PhD Deep vein thrombosis can cause leg pain or swelling but also can occur with no symptoms.
- 43. 43 3/4/2022 Dr. Emad Abu Alrub MD PhD
- 44. 44 3/4/2022 Dr. Emad Abu Alrub MD PhD
- 45. 3/4/2022 Dr. Emad Abu Alrub MD PhD 45
- 46. 3/4/2022 Dr. Emad Abu Alrub MD PhD 46
- 47. Thank you! 47 3/4/2022 Dr. Emad Abu Alrub MD PhD