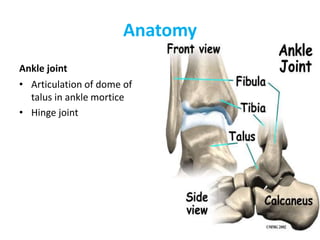
Dr. Manoj Das provides an overview of examining the foot and ankle. The objectives are to assess, diagnose, and treat conditions. The anatomy is complex with 28 bones and 55 joints. The examination involves taking history, observing gait and appearance, palpating for tenderness, and assessing range of motion, neurovascular status, and performing special tests. Key areas to examine include the ankle, subtalar, and first MTP joints as well as the ligaments, tendons and bones of the foot and ankle. A thorough examination is important for accurately diagnosing and treating foot and ankle conditions.