Case
• 35year oldfemale
• Sustained falling down accident from 3m high ladder 2years back
• Landed on her back and lost her consciousness for unknown period of
time
• Since time trauma she had difficulty of walking with limping of left
leg
• She has piercing type of pain over the lower back exacerbated during
movement and decrease but not completely improved during rest
which radiate to the posterior part of left leg
• Other no history of bowel or bladder dysfunction
• No history fever, weight loss
4.
• No historyof headache, abnormal body mov’t
• No history of previous back pain before trauma
• she is a other of 4 and give birth all before accident
• No history of abdominal pain, abdominal swelling or vaginal discharge
• For the above compliant she took amitriptyline 25mg for 2yrs
• Since 5 months back the pain become worse despite amitriptyline
• No history of diabetes mellitus
5.
Physical examination
• GA=ASLin pain
• v/s=BP 110/70 PR=84 RR =20 T=36.9
• MSK:
– There is Gibbs deformity over the lumbar spine, no tenderness
– Healed scar over left gluteal area
• NS:
– conscious and oriented
– No cranial nerve palsy
– power 5/5 on other extrimity
– Normal tone
– Reflex is ++ in ankle, knee and elbow bilaterally
– Pain, touch, vibration sensation is intact
– Coordination is ok
– SLR is positive over the left leg
– Crossed SLR is negative
• What is the cause of her pain?
• How do you manage her ?
6.
Introduction
• Why backpain is a concern in medical community ?
– High cost
– Most common cause of disability in individuals <45 years of age
– Second most common reason for visiting a physician
– More than four out of five people will experience significant back
pain at some point in their lives
• 84 % of adults have low back pain at some time in their lives
• Most of them are self-limited
Terminology
• Spondylosis
– Arthritisof the spine
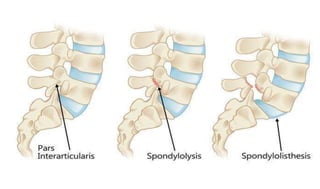
• Spondylolysis
– A fracture in the pars interarticularis where the vertebral body and the posterior
elements protecting the nerves are joined
• Spondylolisthesis
– The injured vertebra to shift or slip forward on the vertebra directly below it
• Spinal stenosis:
– Narrowing of the vertebral canal by bone or soft tissue elements.
• Radiculopathy
– Impairment of a nerve root, usually causing radiating pain, numbness, tingling,
or muscle weakness .
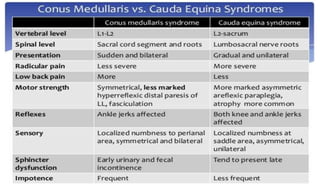
• Cauda equinasyndrome
– Loss of bowel and bladder control
– Numbness in the groin and saddle area of the perineum
– Weakness of the lower extremities
– Spine stenosis or a large herniated disc
Approach to backpain patient
History
• Focus first on features of pain
Mode of onset
Character
Distribution
Associated motor and sensory symptoms
Bladder and bowel control
Exacerbating and remitting factors
History of predisposing factors (e.g., trauma, cancer, osteoporosis)
18.
Type of pain
•Back pain by duration
– Acute LBP → < 6 weeks*
– Sub acute LBP→ between 6 weeks and 12 weeks
– Chronic LBP → > 12 weeks
19.
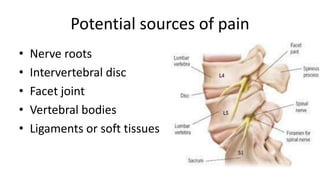
Type of backpain
• Local pain
– injury to pain-sensitive structures that compress or irritate
sensory nerve endings
– The site of the pain is near the affected part of the back
• Pain referred to the back
– From abdominal or pelvic viscera
– Unaffected by posture
– The patient may occasionally complain of back pain only
20.
Cont.
• Pain ofspine origin
– From upper lumbar spine tend to refer pain to the
Lumbar Region, Groin, or Anterior Thighs
– Pain from lower lumbar spine tend to refer to the
buttocks, posterior thighs, or rarely the calves or feet
• Sclerotomal pain VS. radiculopathy?
21.
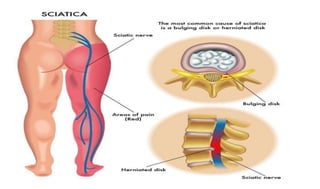
Sciatica
• Pain radiatingdown posterior or lateral leg below the
knee
• The most common cause for sciatica is lumbar disk
herniation
• Symptoms that increase the specificity of sciatica
– Pain that is worse in the leg than in the back
– Typical dermatomal distribution of neurologic symptoms
– Pain that is worse with the Valsalva maneuver
23.
Cont.
• Pain associatedwith muscle spasm
Commonly associated with many spine disorders
The spasms are accompanied by
Abnormal posture
Tense paraspinal muscles
Dull or achy pain in the paraspinal region
24.
“Red flags” inback pain
• Age>55
• History of cancer
• Unexplained weight loss
• Failure to improve with conservative management after 4 weeks of
treatment
• Fever
• Immunosuppression
• Focal midline tenderness
• Bacteremia
• Indwelling catheter
• Iv drug use
• Bowel and bladder dysfunction
25.
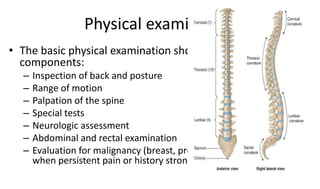
Physical examination
• Thebasic physical examination should include the following
components:
– Inspection of back and posture
– Range of motion
– Palpation of the spine
– Special tests
– Neurologic assessment
– Abdominal and rectal examination
– Evaluation for malignancy (breast, prostate, lymph node exam)
when persistent pain or history strongly suggests systemic disease
26.
• Limited forwardbending
– Paraspinal muscle spasm
• Lateral bending to the side opposite the injured spine
produce pain
• Limited hyperextension of the spine
– Nerve root compression, facet joint pathology, or other bony
spine disease is present
27.
• Pain fromhip disease may mimic the pain of lumbar spine
disease
• Hip pain can be reproduced
– By internal and external rotation at the hip with the knee and hip in
flexion (Patrick's Sign)
– By tapping the heel with the examiner's palm while the leg is
extended (Heel Percussion Sign)
28.
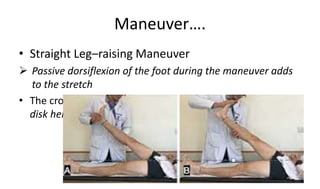
Maneuver….
• Straight Leg–raisingManeuver
Passive dorsiflexion of the foot during the maneuver adds
to the stretch
• The crossed SLR sign is less sensitive but more specific for
disk herniation than the SLR sign
29.
• The ReverseSLR Sign
– Stretches the L2-L4 nerve roots, lumbosacral plexus, and
femoral nerve
• Naffziger’s test
– Pressure on jugular vein on patient lying on back for 10
second
– Back pain reproduce in the case of herniated disc
30.
• Kerning sign
–Meningeal or spinal nerve root irritation
• Hoover test
– Real or malingering
31.
Neurologic examination
• Includes
Focalweakness or muscle atrophy
Focal reflex changes
Diminished sensation in the legs, or
Signs of spinal cord injury
• Alert to the possibility of Breakaway Weakness,
defined as fluctuating strength during muscle testing
32.
• Breakaway weakness
–may be due to pain or a combination of pain and
underlying true weakness
– Breakaway weakness without pain is almost always due
to a lack of effort
– Electromyography during ambiguous condition
Non organic sign(Waddell's signs)
• The most reproducible of these signs are
– Superficial tenderness
– Distracted straight leg raising (ie, discrepancy between seated and supine
straight leg raising tests)
– The observation of patient overreaction during the physical examination
– Non dermatomal distribution of sensory loss,
– Sudden giving way or jerky movements with motor examination
– The presence of multiple Waddell's signs may suggest a behavioral
component to a patient's pain
38.
Laboratory and imaging
•Laboratory studies are rarely needed for the initial evaluation of
nonspecific back pain
• CBC, ESR, urinalysis culture
• No need to investigating, if no serious risk factor
• No needof earlier use of imaging for low back
– meta-analysis of six trials that compared immediate imaging with usual
care for patients
– Without signs or symptoms of infection or malignancy, found no
significant differences in out come
• Imaging scans often have abnormal findings in adults without
low back pain
– Disc herniation on MRI seen in 22 to 67% of asymptomatic adults and
spinal stenosis in 21% of asymptomatic adults over age 60
– Radiologic facet joint osteoarthritis increased with age and there was no
correlation with low back pain
42.
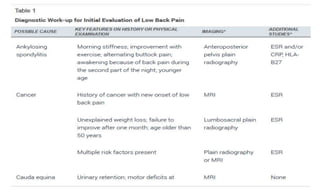
Indication for imaging
•Infection
• Patients with cancer or at high risk of cancer
• Neurologic complication
• Radiculopathy with in need of intervention
• Compression fracture
• Patient with trauma
43.
• Advanced imaging
–MRI without contrast is initial test for most patients with low back pain who require
advanced imaging
– Which can demonstrate normal and pathologic discs, ligaments, nerve roots, epidural
fat, as well as the shape and size of the spinal canal
– MRI is more sensitive and specific than plain radiographs for the detection of spinal
infection and malignancy
– MRI enhancement with gadolinium allows the distinction of scar from disc in patients
with prior back surgery
– In patients who require advanced imaging but cannot have an MRI, we generally
proceed with CT
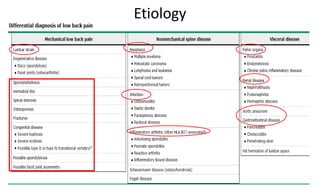
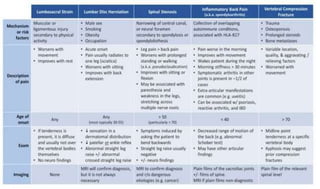
Etiology
• 85% ofpatients have nonspecific low back pain
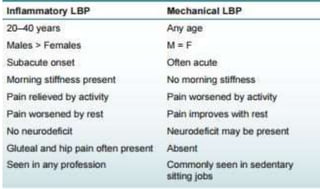
• Etiology of back pain can be categorized as
– Mechanical vs. non mechanical
– Back pain with led pain
– Back pain with out leg pain
– Back pain from visceral causes
– Leg pain with out back pain
Sprains and Strains
•Minor, self-limited injuries
• Lifting a heavy object, a fall, or a sudden deceleration
• Pain is usually confined to the lower back
• No radiation to the buttocks or legs
• Assume unusual postures
53.
Traumatic vertebral fractures
•Results from injuries producing anterior wedging or compression
• Fracture-dislocation or "burst" fracture involving the vertebral body and
posterior elements
• A pars interarticularis fracture of the L5 vertebra is common in case of falls from
a height
• Sudden deceleration in an automobile accident
• Direct injury
• Neurologic impairment is common, and early surgical treatment is indicated
54.
• Metastatic cancer
–The bone is one of the most common sites of metastasis
– A history of cancer
– Metastatic disease from breast, prostate, lung, thyroid, and kidney cancers
account for 80 percent of skeletal metastases
– ~ 60 % of patients with multiple myeloma have skeletal lytic lesions present at
diagnosis
– In patients with a history of cancer, sudden, severe pain raises concern for
pathologic fracture
– Patients may also have neurologic symptoms from either spinal cord
compression or spinal instability
55.
• Spinal epiduralabscess
– Spinal epidural abscess is a rare but serious cause of back pain
– Initial symptoms are often nonspecific
– Over time, localized back pain may be followed by radicular pain and, left
untreated, neurologic deficits
– Risk factors include recent spinal injection or epidural catheter placement,
injection drug use, contagious infections
– Immunocompromised patients may also be at higher risk
– Urgent antibiotic treatment and surgical therapy for those with neurologic
symptoms is required for patients with spinal epidural abscess
56.
• Vertebral osteomyelitis
–Increases with age
– Men >women
– Post procedural from hematogenous spread of bacteremia
– Immunocompromised state and injection drug use
– Acute osteomyelitis typically presents with gradual onset of
symptoms over several days
– Present with back pain but may not have fevers or other
systemic symptoms
– Prompt antibiotic treatment improves outcomes
57.
• Vertebral compressionfracture
– 4 % of low back pain
– From no symptom to acute localize back pain
– There may be no history of preceding trauma
– Advanced age, chronic glucocorticoid use and previous
osteoporotic fracture
– 3 to 4 % of patients with compression fracture will have a
symptomatic disc herniation or spinal stenosis
58.
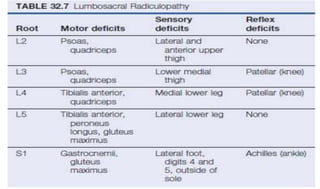
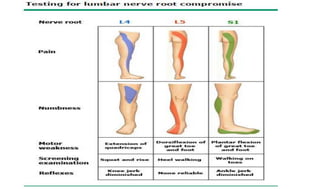
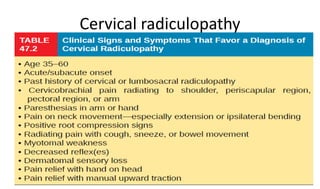
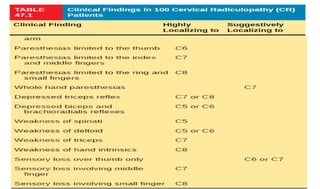
• Radiculopathy
– Resultsfrom degenerative changes in the vertebrae, disc protrusion, and other
causes
– Presentations vary according the level of nerve root or roots involved
– >90 % is L5 and S1 radiculopathies
– Patients present with pain, sensory loss, weakness, and/or reflex changes
consistent with the nerve root involved
– Many patients with symptoms of acute lumbosacral radiculopathy improve
gradually with supportive care
– Sciatica
– SLR positive
59.
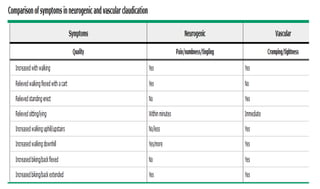
• Spinal stenosis
–Lumbar spinal stenosis is most often multifactorial
– Spondylosis , spondylolistheses, Space-occupying lesions,
traumatic and postoperative fibrosis
– Neurogenic claudication
– Back pain, sensory loss and weakness in the legs
– Rare patients develop a cauda equina syndrome
– Patients often have symptoms only when active
– A trial of conservative, nonsurgical treatment is the initial
therapy for most patients
61.
• Ankylosing spondylitis
–Few (0.5%-1%).
– men under the age of 40 year
– back pain with inflammatory etiology (morning stiffness, improvement with exercise,
pain at night)
– Extra skeletal disease manifestations (eg, uveitis)
• Osteoarthritis
– Facet joint or hip joint
– Commonly presents in patients over the age of 40
– Pain is typically exacerbated by activity and relieved by rest
– Osteoarthritis can lead to spinal stenosis
62.
• Psychological distress
–Who seek financial compensation (malingerers)
– Substance abuse
– Many patients with CLBP have a history of psychiatric illness
– Childhood trauma (physical or sexual abuse) that antedates the
onset of back pain
64.
Management
• Depends on
–Symptom duration
– Potential cause
– Presence or absence of radicular symptoms
– Corresponding anatomical or radiographic abnormalities
65.
Acute back pain
•Self limited
• Pharmacologic
– Acetaminophen
– NSAIDs
– SMRs
• Non pharmacologic
– Heat wrap: improved pain and function
– Massage: improved pain and function
– Acupuncture: improved pain
– Spinal manipulation: improved function
Grade 2C recommendation
66.
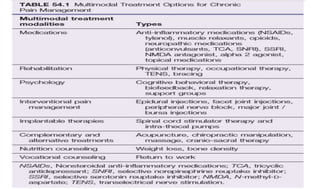
Chronic back pain
•Psychological evaluation and behaviorally based treatment paradigms are
frequently helpful
• Multidisciplinary approach
– Neurology, anesthesiology, physical therapy, psychiatry, psychology, and
primary care physicians
• Goals of therapy
– Improve pain
– Getting a good night’s sleep
– returning to work
67.
• Pharmacologic
– NSAIDs:improved pain
– Opioids: improved pain and function
– Tramadol: improved pain and function
– Buprenorphine (patch or sublingual): improved pain
– Duloxetine: improved pain and function
68.
• Non pharmacologic
–Exercise: improved pain and function
– Motor control exercise: improved pain and function
– Mindfulness-based stress reduction: improved pain and function
– Yoga: improved pain and function
– Progressive relaxation: improved pain and function
70.
Surgical management
• Indicatedfor
– Neurologic deficits
– Cauda equina syndrome or conus medullaris syndrome
– No response with conservative management