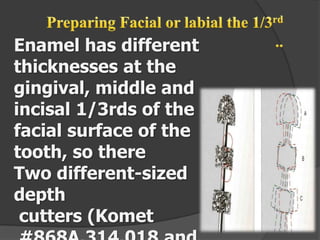
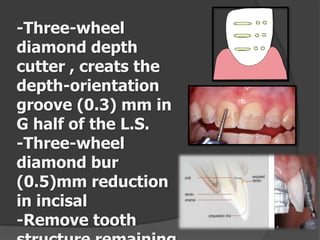
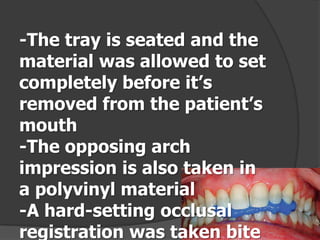
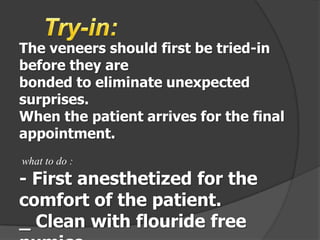
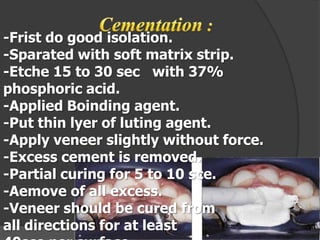
A veneer is a thin restoration placed over tooth surfaces to improve aesthetics or protect damage. Veneers have a translucent quality giving a natural look. Tooth preparation is minimal, reducing enamel by 0.3-0.5mm with a close finish line. Impressions are taken and a try-in ensures proper fit before cementing. Follow-up appointments evaluate tissue response and margins while maintaining good oral hygiene protects the veneers. Bonding uses a micromechanical bond with hydrophilic resins to cement the veneers securely in place.






































![Recent advancements in denture base materials [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/recentadvancementsindenturebasematerialsautosaved-181219143003-thumbnail.jpg?width=640&height=640&fit=bounds)








































