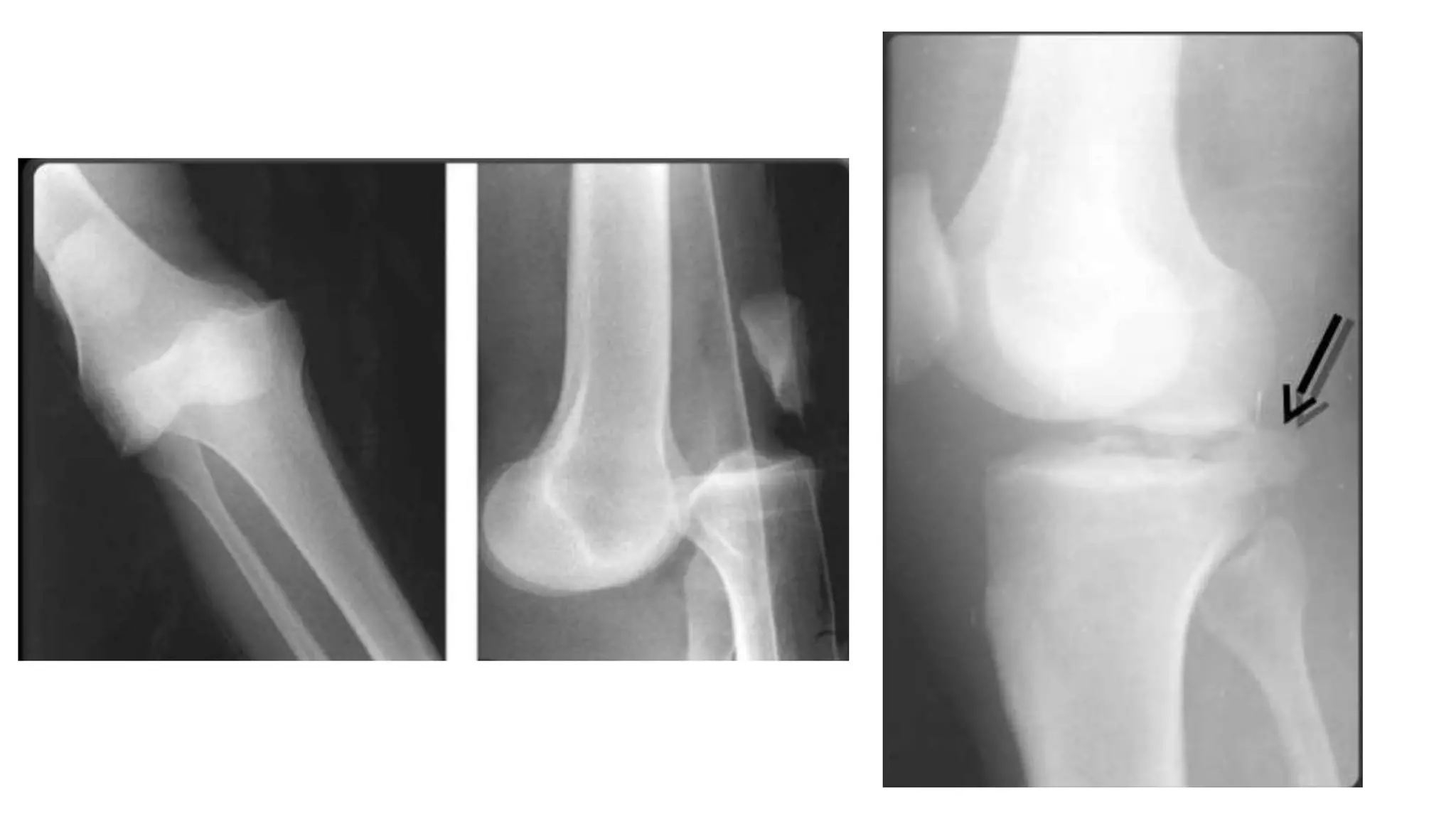
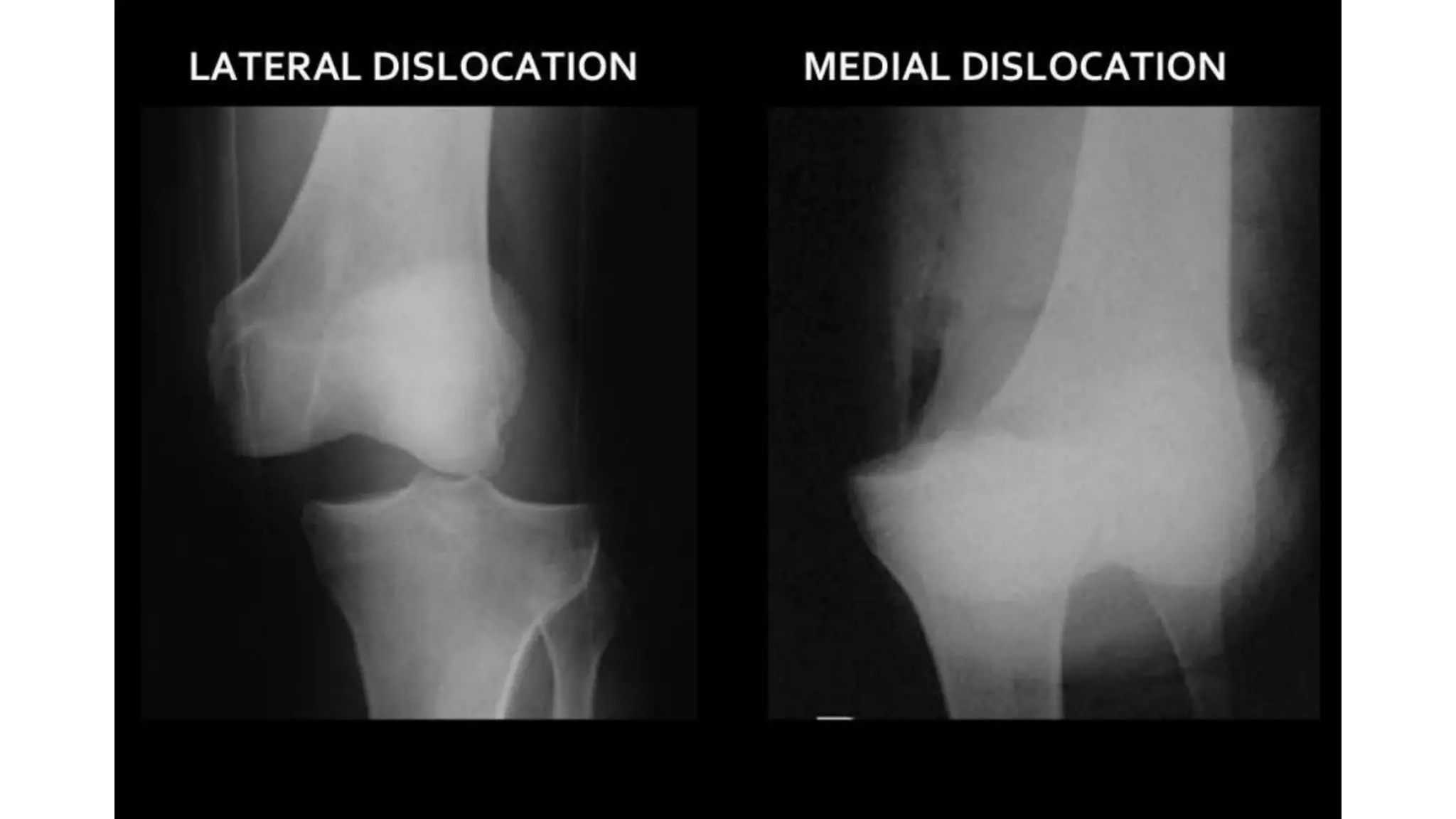
Knee dislocations involve injuries to the ligaments that stabilize the knee joint. The ligaments include the joint capsule, collateral ligaments, and quadriceps tendon. Knee dislocations can occur due to high-energy trauma like car accidents or falls. Classification systems categorize dislocations as anterior, posterior, medial, or lateral. Associated injuries may involve blood vessels or nerves. Treatment depends on the severity of the injury and stability of the knee. Options include closed reduction, splinting, surgery to repair torn ligaments, or reconstructing ligaments with grafts. The goals are to stabilize the knee and allow early rehabilitation.