Downloaded 18 times

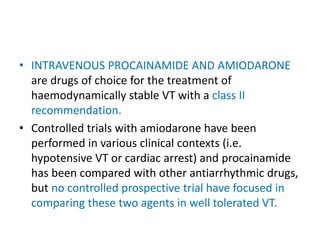














![• Patients were defined as “complex” if they met at least 1 of
the following clinical or lesion characteristics:
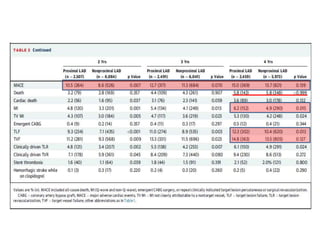
1. Renal insufficiency or failure (defined as creatinine ≥140
mmol/l [1.6 mg/dl]),
2. Left ventricular ejection fraction <30%, the occurrence of an
acuteMI within the previous 72 h,
3. >1 lesion per vessel,
4. ≥2 vessels with stents,
5. Lesion measuring >27 mm,
6. Bifurcation,
7. Bypass grafts,
8. In-stent restenosis,
9. Unprotected left main artery,
10. Lesions with thrombus, or total occlusion (pre-procedure
TIMI [Thrombolysis In Myocardial Infarction] flow grade 0).](https://image.slidesharecdn.com/jcprcamioandprotecttrial-170515073358/85/Jc-prcamio-and-protect-trial-47-320.jpg)

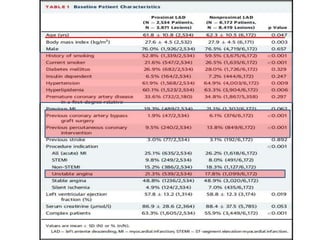
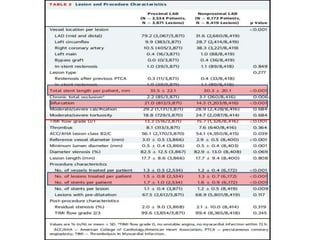
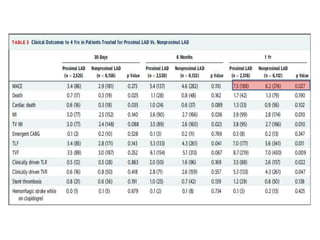

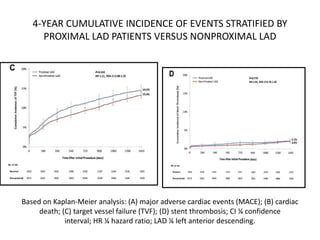




This study compared long-term outcomes of patients who underwent percutaneous coronary intervention (PCI) with drug-eluting stents (DES) for lesions located in the proximal left anterior descending (LAD) artery versus nonproximal LAD lesions. The study analyzed data from 8,709 patients in the PROTECT trial. Results showed no significant differences in rates of death, major adverse cardiac events (MACE), or target vessel failure at 4 years between patients treated for proximal versus nonproximal LAD lesions. Treatment of lesions in the proximal LAD, which supplies a large portion of the left ventricle, did not appear to influence long-term outcomes with modern DES and medical therapy.













































































