Downloaded 393 times






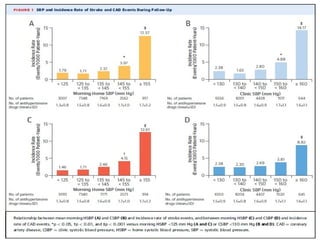
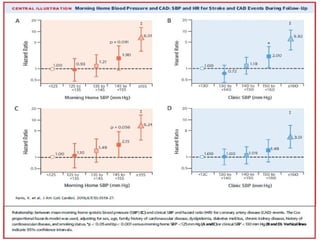
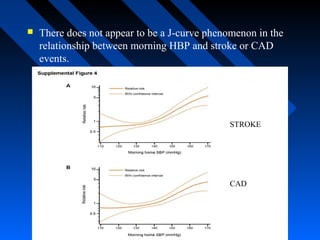

This study analyzed data from over 21,000 Japanese patients to investigate the relationship between blood pressure measurements and cardiovascular outcomes. The results showed that morning home systolic blood pressure was a stronger predictor of coronary artery disease events than clinic blood pressure. There was a graded association between higher morning home systolic blood pressure and increased risk of coronary events. Neither home nor clinic blood pressure measurements showed a J-shaped curve relationship with stroke or coronary artery disease risk.


































































































