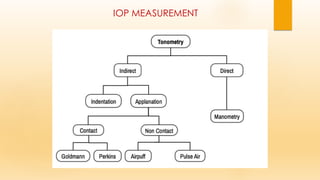
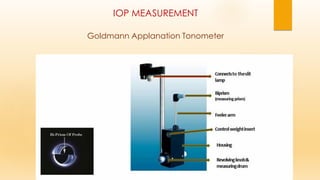
This document discusses intraocular pressure (IOP) measurement. It begins by defining IOP as the pressure exerted by intraocular fluids on the eyeball coats. The normal IOP range is then provided as 10.5-20.5 mm Hg. Factors that can affect IOP levels are described such as aqueous secretion, outflow resistance, and episcleral venous pressure. Common methods of measuring IOP are then outlined, including digital assessment, manometry, indentation tonometry using the Schiotz tonometer, and applanation tonometry using the Goldmann tonometer. Advantages and limitations of each method are summarized.