Molecular basis of IUGR. –
1. Atypical expression of enzymes governed by TGFβ causes the placental apoptosis and altered expression of TGFβ due to hyper alimentation causes impairment of lung function.
2. Crosstalk of cAMP with protein kinases plays a prominent role in the regulation of cortisol levels.
3. Increasing levels of NOD1 proteins leads to development of IUGR by increasing the levels of inflammatory mediators.
4. Increase in leptin synthesis in placental trophoblast cells is associated with IUGR.
A positive history for risk factors of IUGR can raise the problem of an increased surveillance with the specific goal of an early detection of growth insufficiency [23]. Further diagnostic tests could have a better relevance in a selected high-risk population
Serum markers linked to IUGR
The placentation process starts with the migration of trophoblastic cells that invade the walls of spiral arteries and transform them from small caliber high resistant vessels into wide caliber low resistant vessels that deliver blood at low pressure to the intervillous space. Then, the utero-placental circulation develops in two stages: the first stage (until the 10th week of gestation) consists in endovascular plugging of the spiral arteries by trophoblastic cells, subsequently followed by invasion and destruction of the intradecidual spiral arteries; the second stage (between 14-16 weeks of gestation) consists in the invasion of the inner miometrial part of the spiral arteries [27]. The impaired spiral artery transformation is leading to weak development of the utero-placental circulation and is implied in the pathology of preeclampsia and IUGR
Pregnancy associated plasma protein A (PAPP-A), an Insulin–like Growth Factor Binding Protein Protease whose levels depend on placental volume and function, was assessed in several studies with congruent results. In 2000, Ong et al. evaluated 5584 singleton pregnancies at 10-14 weeks of gestation and measured maternal serum free beta human chorionic gonadotropin (β-hCG) and PAPP-A, concluding that low levels of maternal serum PAPP-A or β-hCG were associated with subsequent development of pregnancy
IDD situation in our country has improved
A good number of thyroid disorder patients are either undiagnosed and or untreated
Thyroid disorder in pregnancy- Rate high
As a sound thyroid functioning status is crucial for growth, development in children; reproduction, psychological and general wellbeing in adults, we must be proactive in screening, diagnosing and treating our patients.
A group of physiological abnormalities such as an increase in blood pressure, diabetes, increase in cholesterol levels and obesity is known as Metabolic Syndrome. Women in their pregnancy period are highly prone to this problem. Doctors are taking the issue of metabolic syndrome in obstetric practice seriously as it may risk the pregnancy.
The objectives of this report includes, introducing and looking at the overview of the topic of PCOS, the history of PCOS and what have we learnt about PCOS 1970-2018 etc.
IDD situation in our country has improved
A good number of thyroid disorder patients are either undiagnosed and or untreated
Thyroid disorder in pregnancy- Rate high
As a sound thyroid functioning status is crucial for growth, development in children; reproduction, psychological and general wellbeing in adults, we must be proactive in screening, diagnosing and treating our patients.
A group of physiological abnormalities such as an increase in blood pressure, diabetes, increase in cholesterol levels and obesity is known as Metabolic Syndrome. Women in their pregnancy period are highly prone to this problem. Doctors are taking the issue of metabolic syndrome in obstetric practice seriously as it may risk the pregnancy.
The objectives of this report includes, introducing and looking at the overview of the topic of PCOS, the history of PCOS and what have we learnt about PCOS 1970-2018 etc.
This presentation briefly discuss the polycystic ovary syndrome in terms of pathogenesis, features and management. Then, It moves on to discuss the various guidelines laid down by Endocrine Society in 2013 for the management of patients with polycystic ovary syndrome.
This presentation briefly discuss the polycystic ovary syndrome in terms of pathogenesis, features and management. Then, It moves on to discuss the various guidelines laid down by Endocrine Society in 2013 for the management of patients with polycystic ovary syndrome.
IUGR
Intrauterine growth restriction is said to be present in those babies whose birth weight is below the tength percentile of the average for gestational age.
INCIDENCE
Dysmaturity comprised about one third of low birth weight babies.
In developed countries , its overall incidence is about
3-10%
Term babies (5%)
Post term babies (15%)
CAUSES OF IUGR
The causes of IUGR can be grouped as
Maternal causes
Fetal causes
Placental causes
Uterine and Environmental causes.
MATERNAL CAUSES
Pregnancy weight of mother influences the fetal size
Chronic maternal disease condition
Renal disease condition
Malnutrition
Multiple pregnancy
Hypertensive disorders of pregnancy
Severe anemia
Previous baby suffered iugr etc.
FETAL CAUSES
Chromosomal anomalies
Exposure to an infection
German measles (rubella), cytomegalovirus, herpes simplex, tuberculosis, syphilis, or toxoplasmosis, TB, Malaria, Parvo virus
Birth defects
(cardiovascular, renal, anencephally, limb defect, etc).
• Placenta or umbilical cord defects.
PLACENTAL FACTORS
Uteroplacental Insufficiency
Fetoplacetal Insufficiency
Abruptio placenta
Placenta previa
Post term pregnancy
UTERINE CAUSES
Septate uterus
Fibroid/ myoma uterus
ENVIRONMENTAL CAUSES
High altitude - lower environmental oxygen saturation
Toxins
PATHOPHYSIOLOGY
Due to maternal and placental causes
Decrease in placental transfer of nutrients and oxygen to the fetus
Resulting in reduced fetal body store of lipids, glycogen
Causes neonatal hypoglycemia
Lack of oxygen
Chronic hypoxia that leads to erythropoietin production
Polycythemia etc
CLASSIFICATION OF IUGR
Based On Pathological Processes
I)Type I- Symmetrical
II)Type II- Asymmetrical
SYMMETRICAL
Symmetric IUGR: (33 % of IUGR Infants)
height, weight, head circumference proportional
early pregnancy insult:
commonly due to congenital infection, genetic disorder, or intrinsic factors
reduced no of cells in fetus
normal ponderal index
low risk of perinatal asphyxia
low risk of hypoglycemia
ASYMMETRICAL
later in pregnancy:
commonly due to utero placental insufficiency, maternal malnutrition, hypoxia, or extrinsic factors
low ponderal index
cell number remains same but size is small
increased risk of asphyxia
increased risk of hypoglycemia
CLINICAL FEATURES OF BABY WITH IUGR AT BIRTH
Weight deficit
Large head circumference
Old man look
Cartilaginous ridges on pinna
Dry wrinkled skin
Length remain unaffected
Open eyes
Well defined creases
Alert and active
Normal reflexes Normal cry
Thin umbilical
Scaphoid abdomen
Signs of recent wasting - soft tissue wasting - diminished skin fold thickness - decrease breast tissue - reduced thigh circumference • Signs of long term growth failure - Widened skull sutures, large fontanelles - shortened crown – heel length - delayed development of epiphyses
Normal reflexes Normal cry
Thin umbilical
Scaphoid abdomen
Similar to Intrauterine growth restriction when to deliver by dr alka mukherjee & dr apurva mukherjee nagpur m.s. india (20)
Management of anaemia in pregnancy BY DR ALKA MUKHERJEE DR APURVA MUKHERJEE N...alka mukherjee
Prenatal vitamins typically contain iron. Taking a prenatal vitamin that contains iron can help prevent and treat iron deficiency anemia during pregnancy. In some cases, your health care provider might recommend a separate iron supplement. During pregnancy, you need 27 milligrams of iron a day.
Good nutrition also can prevent iron deficiency anemia during pregnancy. Dietary sources of iron include lean red meat, poultry and fish. Other options include iron-fortified breakfast cereals, prune juice, dried beans and peas.
The iron from animal products, such as meat, is most easily absorbed. To enhance the absorption of iron from plant sources and supplements, pair them with a food or drink high in vitamin C — such as orange juice, tomato juice or strawberries. If you take iron supplements with orange juice, avoid the calcium-fortified variety. Although calcium is an essential nutrient during pregnancy, calcium can decrease iron absorption.
How is iron deficiency anemia during pregnancy treated?
If you are taking a prenatal vitamin that contains iron and you are anemic, your health care provider might recommend testing to determine other possible causes. In some cases, you might need to see a doctor who specializes in treating blood disorders (hematologist). If the cause is iron deficiency, additional supplemental iron might be suggested. If you have a history of gastric bypass or small bowel surgery or are unable to tolerate oral iron, you might need intravenous iron administration. Oral iron is recommended as the first line treatment, with repeated checking of Hb at 2 to 3 weeks after starting treatment to assess compliance, correct administration and response to treatmentOnce Hb reaches the normal range, it is recommended that iron replacement should continue for three months and until at least six weeks postpartumIntravenous (IV) iron is recommended for women who could not tolerate or respond to oral iron, and for those with moderately severe to severe anemia (Hb ≤ 90 g/LHb be measured within 24 to 48 hours after delivery in women with blood loss more than 500 mL, those with uncorrected anemia detected during pregnancy or those with symptoms suggestive of anemia postnatallyOral iron is recommended for women with Hb <100 g/L postpartum, who are hemodynamically stable, asymptomatic or mild symptomatic
Anemia signs and symptoms include:
• Fatigue
• Weakness
• Pale or yellowish skin
• Irregular heartbeats
• Shortness of breath
• Dizziness or lightheadedness
• Chest pain
• Cold hands and feet
• Headache
Keep in mind, however, that symptoms of anemia are often similar to general pregnancy symptoms. Regardless of whether or not you have symptoms, you'll have blood tests to screen for anemia during pregnancy. If you're concerned about your level of fatigue or any other symptoms, talk to your health care provider.
Secondary amenorrhoea by dr alka mukherjee dr apurva mukherjeealka mukherjee
The first step in the evaluation of any patient with secondary amenorrhea is a urine pregnancy test. Every contraceptive method has a failure rate, and anyone who is menstruating is potentially fertile, regardless of age. [5][6]
If the pregnancy test is negative, consider the clinical picture: hirsutism, acne, and a long history of infrequent and irregular menses suggest polycystic ovarian syndrome. By the Rotterdam criteria, a patient may be diagnosed with PCOS if she has two of the following: clinical or chemical hyperandrogenism, oligo- or amenorrhea, or polycystic ovaries on ultrasound. So if a patient has evidence of hirsutism and oligo- or amenorrhea, she can be diagnosed with PCOS without further laboratory testing or imaging.
If history and physical exam are not consistent with PCOS, a TSH should be ordered. Both hyper- and hypothyroidism can lead to menstrual dysfunction.
If TSH is normal, check a serum prolactin. Elevated serum prolactin suggests prolactinoma.
Early pregnancy loss by dr alka mukherjee dr apurva mukherjee nagpur ms indiaalka mukherjee
Early pregnancy loss, or loss of an intrauterine pregnancy within the first trimester, is encountered commonly in clinical practice. Obstetricians and gynecologists should understand the use of various diagnostic tools to differentiate between viable and nonviable pregnancies and offer the full range of therapeutic options to patients, including expectant, medical, and surgical management.
Early pregnancy loss is defined as a nonviable, intrauterine pregnancy with either an empty gestational sac or a gestational sac containing an embryo or fetus without fetal heart activity within the first 12 6/7 weeks of gestation 1. In the first trimester, the terms miscarriage, spontaneous abortion, and early pregnancy loss are used interchangeably, and there is no consensus on terminology in the literature.
Pprom by dr alka mukherjee dr apurva mukherjee nagpur indiaalka mukherjee
Preterm premature rupture of the membranes (PPROM) is a pregnancy complication. In this condition, the sac (amniotic membrane) surrounding your baby breaks (ruptures) before week 37 of pregnancy. Once the sac breaks, you have an increased risk for infection. You also have a higher chance of having your baby born early.
In most cases of PPROM, the cause is not known.
These things may increase risk:
• Having a preterm birth in a previous pregnancy
• Having an infection in your reproductive system
• Vaginal bleeding during pregnancy
• Smoking during pregnancy
Symptoms can occur a bit differently in each pregnancy. They can include:
• A sudden gush of fluid from your vagina
• Leaking of fluid from your vagina
• A feeling of wetness in your vagina or underwear
Call your healthcare provider right away if you have these symptoms.
The symptoms of this health problem may be similar to symptoms of other conditions. See your healthcare provider for a diagnosis.
Diagnosis
• pH (acid-base) balance testing. The pH balance of amniotic fluid is different from vaginal fluid and urine. Your healthcare provider will put the fluid on a test strip to check the balance.
• Looking at a sample under a microscope. When amniotic fluid is dry, it has a fern-like pattern.
• ultrasound exam. This is done to check the amount of amniotic fluid around baby.
Public education on breast cancer hindi by dr alka mukherjee nagpur ms i...alka mukherjee
Abnormal lump — Breast cancer can be discovered when a lump or other change in the breast or armpit is found by a woman herself or by her healthcare provider. In addition to a lump, other abnormal changes may include dimpling of the skin, a change in the size or shape of one breast, retraction (pulling in) of the nipple when it previously pointed outward, or a discoloration of the skin of the breast not related to infection or skin conditions such as psoriasis or eczema.Mammogram — A mammogram is a very low-dose X-ray of the breast. The breast tissue is compressed for the X-ray, which decreases the thickness of the tissue and holds the breast in position, so the radiologist can find abnormalities more accurately. Each breast is compressed between two panels and X-rayed from two directions (top-down and side-to-side) to make sure all the tissue is examined. Mammograms are currently the best screening modality to detect breast cancer. Some mammograms capture images digitally, offering better clarity, the ability to adjust the image, and a decreased likelihood that the woman will need to return on a different day for repeat pictures.
Cancer cervix awareness in hindi by dr alka mukherjee nagpur ms indiaalka mukherjee
Cervical cancer occurs when the cells in the cervix grow abnormally or out of control. The cervix is part of the female reproductive system. The exact cause of cervical cancer is unknown. Certain strains of the human papillomavirus (HPV), a sexually transmitted disease, cause the majority of cervical cancer.
A new vaccine is available to prevent infection against the two types of HPV that are responsible for the majority of cervical cancer cases and the two types of HPV that are responsible for the majority of genital wart cases. A pap smear test is a preventive measure that can detect precancerous or cancerous cells. Precancerous cells are 100% curable.
Telehealth medico legal aspects by dr alka mukherjee nagpur ms indiaalka mukherjee
The term telehealth includes a broad range of technologies and services to provide patient care and improve the healthcare delivery system as a whole. Telehealth is different from telemedicine because it refers to a broader scope of remote healthcare services than telemedicine. While telemedicine refers specifically to remote clinical services, telehealth can refer to remote non-clinical services, such as provider training, administrative meetings, and continuing medical education, in addition to clinical services. According to the World Health Organization, telehealth includes, “Surveillance, health promotion and public health functions.”
Telemedicine involves the use of electronic communications and software to provide clinical services to patients without an in-person visit. Telemedicine technology is frequently used for follow-up visits, management of chronic conditions, medication management, specialist consultation and a host of other clinical services that can be provided remotely via secure video and audio connections.
Evolution and current practices in emergency contraceptives BY DR ALKA MUKHER...alka mukherjee
ey facts
Emergency contraception (EC) can prevent up to over 95% of pregnancies when taken within 5 days after intercourse.
EC can be used in the following situations: unprotected intercourse, concerns about possible contraceptive failure, incorrect use of contraceptives, and sexual assault if without contraception coverage.
Methods of emergency contraception are the copper-bearing intrauterine devices (IUDs) and the emergency contraceptive pills (ECPs).
A copper-bearing IUD is the most effective form of emergency contraception available.
The emergency contraceptive pill regimens recommended by WHO are ulipristal acetate, levonorgestrel, or combined oral contraceptives (COCs) consisting of ethinyl estradiol plus levonorgestrel.
Screening for gestational diabetes an update by dr alka mukherjee nagpur ms i...alka mukherjee
Gestational Diabetes Mellitus (GDM) is defined as any glucose intolerance with the onset or first recognition during pregnancy. This definition helps for diagnosis of unrecognized pre-existing Diabetes also. Hyperglycemia in pregnancy is associated with adverse maternal and prenatal outcome. It is important to screen, diagnose and treat Hyperglycemia in pregnancy to prevent an adverse outcome. There is no international consensus regarding timing of screening method and the optimal cut-off points for diagnosis and intervention of GDM. DIPSI recommends non-fasting Oral Glucose Tolerance Test (OGTT) with 75g of glucose with a cut-off of ≥ 140 mg/dl after 2-hours, whereas WHO (1999) recommends a fasting OGTT after 75g glucose with a cut-off plasma glucose of ≥ 140 mg/dl after 2-hour. The recommendations by ADA/IADPSG for screening women at risk of diabetes is as follows, for first and subsequent trimester at 24-28 weeks a criteria of diagnosis of GDM is made by 75 g OGTT and fasting 5.1mmol/l, 1 hour 10.0mmol/l, 2 hour 8.5mmol/l by universal glucose tolerance testing. Critics of these criteria state that it causes over diagnosis of GDM and unnecessary interventions, the controversy however continues. The ACOG still prefer a 2 step procedure, GCT with 50g glucose non-fasting if value > 7.8mmol/l followed by 3-hour OGTT for confirmation of diagnosis. In conclusion based on Hyperglycemia and Adverse Pregnancy Outcome (HAPO) study as mild degree of dysglycemia are associated with adverse outcome and high prevalence of Type II DM to have international consensus It recommends IADPSG criteria, though controversy exists. The IADPSG criteria is the only outcome based criteria, it has the ability to diagnose and treat GDM earlier, thereby reducing the fetal and maternal complications associated with GDM. This one step method has an advantage of simplicity in execution, more patient friendly, accurate in diagnosis and close to international consensus. Keeping in the mind the diversity and variability of Indian population, judging international criteria may not be conclusive, thus further comparative studies are required on different diagnostic criteria in relation to adverse pregnancy outcomes
Hague convention for inter country adoption by dr alka mukherjee nagpur ms indiaalka mukherjee
The Hague Convention on the Protection of Children and Co-operation in Respect of Intercountry Adoption (Convention) is an international agreement to safeguard intercountry adoptions. Concluded on May 29, 1993 in The Hague, the Netherlands, the Convention establishes international standards of practices for intercountry adoptions. The United States signed the Convention in 1994, and the Convention entered into force for the United States on April 1, 2008The Convention applies to all adoptions by U.S. citizens habitually resident in the United States of children habitually resident in any country outside of the United States that is a party to the Convention (Convention countries). Adopting a child from a Convention country is similar in many ways to adopting a child from a country not party to the Convention. However, there are some key differences. In particular, those seeking to adopt may receive greater protections if they adopt from a Convention country.
The Convention requires that countries who are party to it establish a Central Authority to be the authoritative source of information and point of contact in that country. The Department of State is the U.S. Central Authorityfor the Convention.
The Convention aims to prevent the abduction, sale of, or trafficking in children, and it works to ensure that intercountry adoptions are in the best interests of children.
The Convention recognizes intercountry adoption as a means of offering the advantage of a permanent home to a child when a suitable family has not been found in the child's country of origin. It enables intercountry adoption to take place when, among other steps:
1. The child has been deemed eligible for adoption by the child's country of origin; and
2. Due consideration has been given to finding an adoption placement for the child in its country of origin.
The role of judiciary & the legal procedure in an adoption case by dr alka mu...alka mukherjee
Central Adoption Resource Authority (CARA) is the nodal agency to monitor and regulate in-country and intra-country adoption and is a part of Ministry of Women and child care.
Following are the certain essential conditions in order to be eligible to adopt a child:
• The procedure for adoption is different in case of Indian citizen, NRI or a foreign citizen and a child can be adopted by any of the three.
• Irrespective of their gender or marital status, any person is eligible to adopt.
• Provided that a couple is adopting a child, they should have completed two years of stable marriage and both should agree for the adoption.
• 25 years should be the minimum age difference between the child and the adoptive parents.
WHEN CAN A CHILD BE ELIGIBLE TO BE ADOPTED?
• Any orphan, surrendered or abandoned child is legally declared free for adoption by the child welfare committee as per the guidelines of the Central Government of India.
• A child without a legal parent or a guardian or the parents are not capable of taking care of the child anymore is said to be an orphan.
• When a child is deserted or unaccompanied by parents or a guardian and the child welfare committee has declared the child to be abandoned, a child is considered to be abandoned.
• Renounce on account of physical, social and emotional factors that are beyond the control of parents or the guardian is called a surrendered child as declared by the child welfare committee.
• In case of adoption, a child requires to be “legally free”. A child is considered to be legally free if even after trying their level best the police fails to find the true parent or guardian of the child.
WHAT ARE THE NORMAL CONDITIONS TO BE FULFILLED BY PARENTS?
• The adoptive parents need to be mentally, physically and emotionally stable.
• The adoptive parents should be financially stable.
• The adoptive parents should not be suffering from any life- threatening diseases.
• Apart from cases of special needs children, couples with three or more kids are not allowed for adoption.
• A single female is allowed to adopt a child of any gender but a single male is not allowed to adopt a girl child.
• The maximum age limit of a single parents should be 55 years.
Laws , rules & regulations governing adoptions in india by dr alka mukherjee ...alka mukherjee
ADOPTION IN INDIA
The custom and practice of adoption in India dates back to the ancient times. Although the act of adoption remains the same, the objective with which this act is carried out has differed. It usually ranged from the humanitarian motive of caring and bringing up a neglected or destitute child, to a natural desire for a kid as an object of affection, a caretaker in old age, and an heir after death.[iii]
But since adoption comes under the ambit of personal laws, there has not been a scope in the Indian scenario to incorporate a uniform law among the different communities which consist of this melting pot. Hence, this law is governed by various personal laws of different religions.
Adoption is not permitted in the personal laws of Muslims, Christians, Parsis and Jews in India. Hence they usually opt for guardianship of a child through the Guardians and Wards Act, 1890.
Indian citizens who are Hindus, Jains, Sikhs, or Buddhists are allowed to formally adopt a child. The adoption is under the Hindu Adoption and Maintenance Act of 1956 that was enacted in India as a part of the Hindu Code Bills. It brought about a few reforms that liberalized the institution of adoption.
Tuberculosis in prenancy by dr alka mukherjee dr apurva mukherjee nagpur ms i...alka mukherjee
Prevention of Tuberculosis
The BCG vaccine has been incorporated into the National immunization policy of many countries, especially the high burden countries, thereby conferring active immunity from childhood. Nonimmune women travelling to tuberculosis endemic countries should also be vaccinated. It must, however, be noted that the vaccine is contraindicated in pregnancy [72].
The prevention, however, goes beyond this as it is essentially a disease of poverty. Improved living condition is, therefore, encouraged with good ventilation, while overcrowding should be avoided. Improvement in nutritional status is another important aspect of the prevention.
Pregnant women living with HIV are at higher risk for TB, which can adversely influence maternal and perinatal outcomes [73]. As much as 1.1 million people were diagnosed with the co-infection in 2009 alone [2]. Primary prevention of HIV/AIDS is, therefore, another major step in the prevention of tuberculosis in pregnancy. Screening of all pregnant women living with HIV for active tuberculosis is recommended even in the absence of overt clinical signs of the disease.
Isoniazid preventive therapy (IPT) is another innovation of the World Health Organisation that is aimed at reducing the infection in HIV positive pregnant women based on evidence and experience and it has been concluded that pregnancy should not be a contraindication to receiving IPT. However, patient's individualisation and rational clinical judgement is required for decisions such as the best time to provide IPT to pregnant women
Torch infections during pregnancy by dr alka mukherjee nagpur ms indiaalka mukherjee
TORCH Syndrome refers to infection of a developing fetus or newborn by any of a group of infectious agents. "TORCH" is an acronym meaning (T)oxoplasmosis, (O)ther Agents, (R)ubella (also known as German Measles), (C)ytomegalovirus, and (H)erpes Simplex. Infection with any of these agents (i.e., Toxoplasma gondii, rubella virus, cytomegalovirus, herpes simplex viruses) may cause a constellation of similar symptoms in affected newborns. These may include fever; difficulties feeding; small areas of bleeding under the skin, causing the appearance of small reddish or purplish spots; enlargement of the liver and spleen (hepatosplenomegaly); yellowish discoloration of the skin, whites of the eyes, and mucous membranes (jaundice); hearing impairment; abnormalities of the eyes; and/or other symptoms and findings. Each infectious agent may also result in additional abnormalities that may be variable, depending upon a number of factors (e.g., stage of fetal development
How to develope your personality by dr alka mukherjee nagpur ms indiaalka mukherjee
Personality is what makes a person a unique person, and it is recognizable soon after birth. A child's personality has several components: temperament, environment, and character. Temperament is the set of genetically determined traits that determine the child's approach to the world and how the child learns about the world. There are no genes that specify personality traits, but some genes do control the development of the nervous system, which in turn controls behavior.
A second component of personality comes from adaptive patterns related to a child's specific environment. Most psychologists agree that these two factors—temperament and environment—influence the development of a person's personality the most. Temperament, with its dependence on genetic factors, is sometimes referred to as "nature," while the environmental factors are called "nurture."
While there is still controversy as to which factor ranks higher in affecting personality development, all experts agree that high-quality parenting plays a critical role in the development of a child's personality. When parents understand how their child responds to certain situations, they can anticipate issues that might be problematic for their child. They can prepare the child for the situation or in some cases they may avoid a potentially difficult situation altogether. Parents who know how to adapt their parenting approach to the particular temperament of their child can best provide guidance and ensure the successful development of their child's personality.
Finally, the third component of personality is character—the set of emotional, cognitive, and behavioral patterns learned from experience that determines how a person thinks, feels, and behaves. A person's character continues to evolve throughout life, although much depends on inborn traits and early experiences. Character is also dependent on a person's moral development .
Personality by dr alka mukherjee nagpur ms indiaalka mukherjee
The word personality itself stems from the Latin word persona, which refers to a theatrical mask worn by performers in order to either project different roles or disguise their identities.
At its most basic, personality is the characteristic patterns of thoughts, feelings, and behaviors that make a person unique. It is believed that personality arises from within the individual and remains fairly consistent throughout life.
While there are many different definitions of personality, most focus on the pattern of behaviors and characteristics that can help predict and explain a person's behavior.
Explanations for personality can focus on a variety of influences, ranging from genetic explanations for personality traits to the role of the environment and experience in shaping an individual's personality.
Qualitative blood loss in obstetric hemorrhage by dr alka mukherjee indiaalka mukherjee
• Quantitative methods of measuring obstetric blood loss have been shown to be more accurate than visual estimation in determining obstetric blood loss.
• Studies that have compared visual estimation to quantitative measurement have found that visual estimation is more likely to underestimate the actual blood loss when volumes are high and overestimate when volumes are low.
• Although quantitative measurement is more accurate than visual estimation for identifying obstetric blood loss, the effectiveness of quantitative blood loss measurement on clinical outcomes has not been demonstrated.
• Implementation of quantitative assessment of blood loss includes the following two items: 1) use of direct measurement of obstetric blood loss (quantitative blood loss) and 2) protocols for collecting and reporting a cumulative record of blood loss postdelivery.
Dysmenorrhea and related disorders by dr alka mukherjee dr apurva mukherjee n...alka mukherjee
Dysmenorrhea is a common symptom secondary to various gynecological disorders, but it is also represented in most women as a primary form of disease. Pain associated with dysmenorrhea is caused by hypersecretion of prostaglandins and an increased uterine contractility. The primary dysmenorrhea is quite frequent in young women and remains with a good prognosis, even though it is associated with low quality of life. The secondary forms of dysmenorrhea are associated with endometriosis and adenomyosis and may represent the key symptom. The diagnosis is suspected on the basis of the clinical history and the physical examination and can be confirmed by ultrasound, which is very useful to exclude some secondary causes of dysmenorrhea, such as endometriosis and adenomyosis. The treatment options include non-steroidal anti-inflammatory drugs alone or combined with oral contraceptives or progestins.
Dyspareunia & vulvodynia by dr alka mukherjee dr apurva mukherjee nagpur m.s....alka mukherjee
Pain during or after sexual intercourse is known as dyspareunia. Although this problem can affect men, it is more common in women. Women with dyspareunia may have pain in the vagina, clitoris or labia. There are numerous causes of dyspareunia, many of which are treatable. Common causes include the following:
• Vaginal dryness
• Atrophic vaginitis, a common condition causing thinning of the vaginal lining in postmenopausal women
• Side effects of drugs such as antihistamines and tamoxifen (Nolvadex and other brands)
• An allergic reaction to clothing, spermicides or douches
• Endometriosis, an often painful condition in which tissue from the uterine lining migrates and grows abnormally inside the pelvis
• Inflammation of the area surrounding the vaginal opening, called vulvar vestibulitis
• Skin diseases, such as lichen planus and lichen sclerosus, affecting the vaginal area
• Urinary tract infections, vaginal yeast infections, or sexually transmitted diseases
• Psychological trauma, often stemming from a past history of sexual abuse or trauma
Symptoms
Women with dyspareunia may feel superficial pain at the entrance of the vagina, or deeper pain during penetration or thrusting of the penis. Some women also may experience severe tightening of the vaginal muscles during penetration, a condition called vaginismus.
Chronic pelvic pain by dr alka mukherjee dr apurva mukherjee nagpur m.s. indiaalka mukherjee
Chronic pelvic pain in women is defined as persistent, noncyclic pain perceived to be in structures related to the pelvis and lasting more than six months. Often no specific etiology can be identified, and it can be conceptualized as a chronic regional pain syndrome or functional somatic pain syndrome. It is typically associated with other functional somatic pain syndromes (e.g., irritable bowel syndrome, nonspecific chronic fatigue syndrome) and mental health disorders (e.g., posttraumatic stress disorder, depression). Diagnosis is based on findings from the history and physical examination. Pelvic ultrasonography is indicated to rule out anatomic abnormalities. Referral for diagnostic evaluation of endometriosis by laparoscopy is usually indicated in severe cases. Curative treatment is elusive, and evidence-based therapies are limited. Patient engagement in a biopsychosocial approach is recommended, with treatment of any identifiable disease process such as endometriosis, interstitial cystitis/painful bladder syndrome, and comorbid depression. Potentially beneficial medications include depot medroxyprogesterone, gabapentin, nonsteroidal anti-inflammatory drugs, and gonadotropin-releasing hormone agonists with add-back hormone therapy. Pelvic floor physical therapy may be helpful. Behavioral therapy is an integral part of treatment. In select cases, neuromodulation of sacral nerves may be appropriate. Hysterectomy may be considered as a last resort if pain seems to be of uterine origin, although significant improvement occurs in only about one-half of cases. Chronic pelvic pain should be managed with a collaborative, patient-centered approach.
Ozempic: Preoperative Management of Patients on GLP-1 Receptor Agonists Saeid Safari
Preoperative Management of Patients on GLP-1 Receptor Agonists like Ozempic and Semiglutide
ASA GUIDELINE
NYSORA Guideline
2 Case Reports of Gastric Ultrasound
Title: Sense of Smell
Presenter: Dr. Faiza, Assistant Professor of Physiology
Qualifications:
MBBS (Best Graduate, AIMC Lahore)
FCPS Physiology
ICMT, CHPE, DHPE (STMU)
MPH (GC University, Faisalabad)
MBA (Virtual University of Pakistan)
Learning Objectives:
Describe the primary categories of smells and the concept of odor blindness.
Explain the structure and location of the olfactory membrane and mucosa, including the types and roles of cells involved in olfaction.
Describe the pathway and mechanisms of olfactory signal transmission from the olfactory receptors to the brain.
Illustrate the biochemical cascade triggered by odorant binding to olfactory receptors, including the role of G-proteins and second messengers in generating an action potential.
Identify different types of olfactory disorders such as anosmia, hyposmia, hyperosmia, and dysosmia, including their potential causes.
Key Topics:
Olfactory Genes:
3% of the human genome accounts for olfactory genes.
400 genes for odorant receptors.
Olfactory Membrane:
Located in the superior part of the nasal cavity.
Medially: Folds downward along the superior septum.
Laterally: Folds over the superior turbinate and upper surface of the middle turbinate.
Total surface area: 5-10 square centimeters.
Olfactory Mucosa:
Olfactory Cells: Bipolar nerve cells derived from the CNS (100 million), with 4-25 olfactory cilia per cell.
Sustentacular Cells: Produce mucus and maintain ionic and molecular environment.
Basal Cells: Replace worn-out olfactory cells with an average lifespan of 1-2 months.
Bowman’s Gland: Secretes mucus.
Stimulation of Olfactory Cells:
Odorant dissolves in mucus and attaches to receptors on olfactory cilia.
Involves a cascade effect through G-proteins and second messengers, leading to depolarization and action potential generation in the olfactory nerve.
Quality of a Good Odorant:
Small (3-20 Carbon atoms), volatile, water-soluble, and lipid-soluble.
Facilitated by odorant-binding proteins in mucus.
Membrane Potential and Action Potential:
Resting membrane potential: -55mV.
Action potential frequency in the olfactory nerve increases with odorant strength.
Adaptation Towards the Sense of Smell:
Rapid adaptation within the first second, with further slow adaptation.
Psychological adaptation greater than receptor adaptation, involving feedback inhibition from the central nervous system.
Primary Sensations of Smell:
Camphoraceous, Musky, Floral, Pepperminty, Ethereal, Pungent, Putrid.
Odor Detection Threshold:
Examples: Hydrogen sulfide (0.0005 ppm), Methyl-mercaptan (0.002 ppm).
Some toxic substances are odorless at lethal concentrations.
Characteristics of Smell:
Odor blindness for single substances due to lack of appropriate receptor protein.
Behavioral and emotional influences of smell.
Transmission of Olfactory Signals:
From olfactory cells to glomeruli in the olfactory bulb, involving lateral inhibition.
Primitive, less old, and new olfactory systems with different path
HOT NEW PRODUCT! BIG SALES FAST SHIPPING NOW FROM CHINA!! EU KU DB BK substit...GL Anaacs
Contact us if you are interested:
Email / Skype : kefaya1771@gmail.com
Threema: PXHY5PDH
New BATCH Ku !!! MUCH IN DEMAND FAST SALE EVERY BATCH HAPPY GOOD EFFECT BIG BATCH !
Contact me on Threema or skype to start big business!!
Hot-sale products:
NEW HOT EUTYLONE WHITE CRYSTAL!!
5cl-adba precursor (semi finished )
5cl-adba raw materials
ADBB precursor (semi finished )
ADBB raw materials
APVP powder
5fadb/4f-adb
Jwh018 / Jwh210
Eutylone crystal
Protonitazene (hydrochloride) CAS: 119276-01-6
Flubrotizolam CAS: 57801-95-3
Metonitazene CAS: 14680-51-4
Payment terms: Western Union,MoneyGram,Bitcoin or USDT.
Deliver Time: Usually 7-15days
Shipping method: FedEx, TNT, DHL,UPS etc.Our deliveries are 100% safe, fast, reliable and discreet.
Samples will be sent for your evaluation!If you are interested in, please contact me, let's talk details.
We specializes in exporting high quality Research chemical, medical intermediate, Pharmaceutical chemicals and so on. Products are exported to USA, Canada, France, Korea, Japan,Russia, Southeast Asia and other countries.
Lung Cancer: Artificial Intelligence, Synergetics, Complex System Analysis, S...Oleg Kshivets
RESULTS: Overall life span (LS) was 2252.1±1742.5 days and cumulative 5-year survival (5YS) reached 73.2%, 10 years – 64.8%, 20 years – 42.5%. 513 LCP lived more than 5 years (LS=3124.6±1525.6 days), 148 LCP – more than 10 years (LS=5054.4±1504.1 days).199 LCP died because of LC (LS=562.7±374.5 days). 5YS of LCP after bi/lobectomies was significantly superior in comparison with LCP after pneumonectomies (78.1% vs.63.7%, P=0.00001 by log-rank test). AT significantly improved 5YS (66.3% vs. 34.8%) (P=0.00000 by log-rank test) only for LCP with N1-2. Cox modeling displayed that 5YS of LCP significantly depended on: phase transition (PT) early-invasive LC in terms of synergetics, PT N0—N12, cell ratio factors (ratio between cancer cells- CC and blood cells subpopulations), G1-3, histology, glucose, AT, blood cell circuit, prothrombin index, heparin tolerance, recalcification time (P=0.000-0.038). Neural networks, genetic algorithm selection and bootstrap simulation revealed relationships between 5YS and PT early-invasive LC (rank=1), PT N0—N12 (rank=2), thrombocytes/CC (3), erythrocytes/CC (4), eosinophils/CC (5), healthy cells/CC (6), lymphocytes/CC (7), segmented neutrophils/CC (8), stick neutrophils/CC (9), monocytes/CC (10); leucocytes/CC (11). Correct prediction of 5YS was 100% by neural networks computing (area under ROC curve=1.0; error=0.0).
CONCLUSIONS: 5YS of LCP after radical procedures significantly depended on: 1) PT early-invasive cancer; 2) PT N0--N12; 3) cell ratio factors; 4) blood cell circuit; 5) biochemical factors; 6) hemostasis system; 7) AT; 8) LC characteristics; 9) LC cell dynamics; 10) surgery type: lobectomy/pneumonectomy; 11) anthropometric data. Optimal diagnosis and treatment strategies for LC are: 1) screening and early detection of LC; 2) availability of experienced thoracic surgeons because of complexity of radical procedures; 3) aggressive en block surgery and adequate lymph node dissection for completeness; 4) precise prediction; 5) adjuvant chemoimmunoradiotherapy for LCP with unfavorable prognosis.
Ethanol (CH3CH2OH), or beverage alcohol, is a two-carbon alcohol
that is rapidly distributed in the body and brain. Ethanol alters many
neurochemical systems and has rewarding and addictive properties. It
is the oldest recreational drug and likely contributes to more morbidity,
mortality, and public health costs than all illicit drugs combined. The
5th edition of the Diagnostic and Statistical Manual of Mental Disorders
(DSM-5) integrates alcohol abuse and alcohol dependence into a single
disorder called alcohol use disorder (AUD), with mild, moderate,
and severe subclassifications (American Psychiatric Association, 2013).
In the DSM-5, all types of substance abuse and dependence have been
combined into a single substance use disorder (SUD) on a continuum
from mild to severe. A diagnosis of AUD requires that at least two of
the 11 DSM-5 behaviors be present within a 12-month period (mild
AUD: 2–3 criteria; moderate AUD: 4–5 criteria; severe AUD: 6–11 criteria).
The four main behavioral effects of AUD are impaired control over
drinking, negative social consequences, risky use, and altered physiological
effects (tolerance, withdrawal). This chapter presents an overview
of the prevalence and harmful consequences of AUD in the U.S.,
the systemic nature of the disease, neurocircuitry and stages of AUD,
comorbidities, fetal alcohol spectrum disorders, genetic risk factors, and
pharmacotherapies for AUD.
NVBDCP.pptx Nation vector borne disease control programSapna Thakur
NVBDCP was launched in 2003-2004 . Vector-Borne Disease: Disease that results from an infection transmitted to humans and other animals by blood-feeding arthropods, such as mosquitoes, ticks, and fleas. Examples of vector-borne diseases include Dengue fever, West Nile Virus, Lyme disease, and malaria.
These lecture slides, by Dr Sidra Arshad, offer a quick overview of physiological basis of a normal electrocardiogram.
Learning objectives:
1. Define an electrocardiogram (ECG) and electrocardiography
2. Describe how dipoles generated by the heart produce the waveforms of the ECG
3. Describe the components of a normal electrocardiogram of a typical bipolar leads (limb II)
4. Differentiate between intervals and segments
5. Enlist some common indications for obtaining an ECG
Study Resources:
1. Chapter 11, Guyton and Hall Textbook of Medical Physiology, 14th edition
2. Chapter 9, Human Physiology - From Cells to Systems, Lauralee Sherwood, 9th edition
3. Chapter 29, Ganong’s Review of Medical Physiology, 26th edition
4. Electrocardiogram, StatPearls - https://www.ncbi.nlm.nih.gov/books/NBK549803/
5. ECG in Medical Practice by ABM Abdullah, 4th edition
6. ECG Basics, http://www.nataliescasebook.com/tag/e-c-g-basics
Tom Selleck Health: A Comprehensive Look at the Iconic Actor’s Wellness Journeygreendigital
Tom Selleck, an enduring figure in Hollywood. has captivated audiences for decades with his rugged charm, iconic moustache. and memorable roles in television and film. From his breakout role as Thomas Magnum in Magnum P.I. to his current portrayal of Frank Reagan in Blue Bloods. Selleck's career has spanned over 50 years. But beyond his professional achievements. fans have often been curious about Tom Selleck Health. especially as he has aged in the public eye.
Follow us on: Pinterest
Introduction
Many have been interested in Tom Selleck health. not only because of his enduring presence on screen but also because of the challenges. and lifestyle choices he has faced and made over the years. This article delves into the various aspects of Tom Selleck health. exploring his fitness regimen, diet, mental health. and the challenges he has encountered as he ages. We'll look at how he maintains his well-being. the health issues he has faced, and his approach to ageing .
Early Life and Career
Childhood and Athletic Beginnings
Tom Selleck was born on January 29, 1945, in Detroit, Michigan, and grew up in Sherman Oaks, California. From an early age, he was involved in sports, particularly basketball. which played a significant role in his physical development. His athletic pursuits continued into college. where he attended the University of Southern California (USC) on a basketball scholarship. This early involvement in sports laid a strong foundation for his physical health and disciplined lifestyle.
Transition to Acting
Selleck's transition from an athlete to an actor came with its physical demands. His first significant role in "Magnum P.I." required him to perform various stunts and maintain a fit appearance. This role, which he played from 1980 to 1988. necessitated a rigorous fitness routine to meet the show's demands. setting the stage for his long-term commitment to health and wellness.
Fitness Regimen
Workout Routine
Tom Selleck health and fitness regimen has evolved. adapting to his changing roles and age. During his "Magnum, P.I." days. Selleck's workouts were intense and focused on building and maintaining muscle mass. His routine included weightlifting, cardiovascular exercises. and specific training for the stunts he performed on the show.
Selleck adjusted his fitness routine as he aged to suit his body's needs. Today, his workouts focus on maintaining flexibility, strength, and cardiovascular health. He incorporates low-impact exercises such as swimming, walking, and light weightlifting. This balanced approach helps him stay fit without putting undue strain on his joints and muscles.
Importance of Flexibility and Mobility
In recent years, Selleck has emphasized the importance of flexibility and mobility in his fitness regimen. Understanding the natural decline in muscle mass and joint flexibility with age. he includes stretching and yoga in his routine. These practices help prevent injuries, improve posture, and maintain mobilit
Tom Selleck Health: A Comprehensive Look at the Iconic Actor’s Wellness Journey
Intrauterine growth restriction when to deliver by dr alka mukherjee & dr apurva mukherjee nagpur m.s. india
1. Dr Alka Mukherjee Nagpur 1
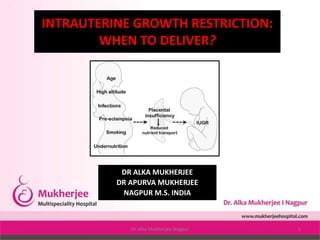
INTRAUTERINE GROWTH RESTRICTION:
WHEN TO DELIVER?
DR ALKA MUKHERJEE
DR APURVA MUKHERJEE
NAGPUR M.S. INDIA
2. DR ALKA MUKHERJEE
MBBS DGO FICOG FICMCH PGDCR PGDMLS MA(PSY)
Director & Consultant At Mukherjee Multispecialty
Hospital
MMC ACCREDITATED SPEAKER
MMC OBSERVER MMC MAO – 01017 / 2016
Present Position
Director of Mukherjee Multispecialty Hospital
Hon.Secretary INTERNATIONAL COUNCIL FOR HUMAN
RIGHTS
Hon.Secretary NARCHI NAGPUR CHAPTER (2018-2020)
Hon.Secretary AMWN (2018-2021)
Hon.Secretary ISOPARB (2019-2021)
Organizing secretary AMWICON – 2019
Life member, IMA, NOGS, NARCHI, AMWN &
Menopause Society, India, Indian medico-legal &
ethics association(IMLEA), ISOPARB, HUMAN RIGHTS
Founder Member of South Rapid Action Group,
Nagpur.
On Board of Super Specialty, GMC, IGGMC, AIIMS
Nagpur, NKPSIMS, ESIS and Treasury, Nagpur for “
WOMEN SEXUAL HARASSMENT COMMITTEE.”
mukherjeehospital@yahoo.com
www.mukherjeehospital.com
https://www.facebook.com/
Mukherjee Multispeciality
https://www.instagram.com/
Achievement
Winner of NOGS GOLD MEDAL – 2017-18
Winner of BEST COUPLE AWARD in Social
Work - 2014
VIDARBHA RATNA PURASKAR - 2019
Past Position
Vice President of NOGS(2016-2017)
Organizing joint secretary ENDO-GYN
Vice President IMA Nagpur (2017-2018)
Organizing joint secretary ENDO-GYN 2019
3. INTRODUCTION
• Pregnancies with intrauterine growth restriction (IUGR) - a
major obstetric problem
• Associated with increased neonatal morbidity and mortality
• Adverse intrauterine environment may increase disease risk
of hypertension, diabetes, coronary heart disease, and
stroke in adulthood.
• Affects up to 10% of all pregnancies.
• Majority of such pregnancies will have a physiologically
normal foetus that is simply small for gestational age (sga),
the ability to differentiate such a foetus from the
pathologically growth-restricted foetus is limited.”
4.
5. • The management of growth restriction depends on the
cause. In 40% of cases, however, the cause is not definite
which also necessitates management.
9. PATHO-PHYSIOLOGY OF
IUGR
• IUGR occurs when gas exchange and nutrient delivery to the fetus
are not sufficient to allow it to thrive in utero.
• This process can occur primarily because of maternal disease
causing decreased oxygen-carrying capacity (eg, cyanotic heart
disease, smoking, hemoglobinopathy),
• A dysfunctional oxygen delivery system secondary to maternal
vascular disease (eg, diabetes with vascular disease, hypertension,
autoimmune disease affecting the vessels leading to the placenta),
• Or placental damage resulting from maternal disease (eg, smoking,
thrombophilia, various autoimmune diseases).
• Evaluation of causative factors for intrinsic disorders leading to poor
growth may include a fetal karyotype, maternal serology for
infectious processes, and an environmental exposure history.
10.
11.
12.
13.
14. Perinatal Implications
• IUGR causes a spectrum of perinatal complications:
• fetal morbidity and mortality,
• iatrogenic prematurity,
• fetal compromise in labor,
• need for induction of labor, and
• cesarean delivery.
• a increase in late fetal deaths among very small fetuses.
• Almost 40 0% of stillborn fetuses not malformed are SGA.
• Fetuses with IUGR who survive the compromised I-U
environment - increased risk for neonatal morbidity -
increased rates of necrotizing enterocolitis, renal failure
thrombocytopenia, temperature instability - occur as a result
of the alteration of normal fetal physiology in utero.
15.
16. The brain-sparing effect
• With limited nutritional reserve, the fetus redistributes
blood flow to sustain function and to help in the
development of vital organs - and results in increased
relative blood flow to the brain, heart, adrenals, and
placenta, with diminished relative flow to the bone marrow,
muscles, lungs, gastrointestinal (GI) tract, and kidneys - may
result in different fetal growth patterns.
• Symmetrically small fetuses - early global insult (eg,
aneuploidy, viral infection, fetal alcohol syndrome).
• Asymmetrically small fetuses -small secondary to an
imposed restriction in nutrient and gas exchange.
17.
18. • Greater predisposition to develop a metabolic syndrome later in
life - obesity, hypertension, hypercholesterolemia, cardiovascular
disease, and type 2 diabetes - thrifty GENE HYPOTHESIS -
intrauterine malnutrition results in insulin resistance, loss of
pancreatic beta-cell mass, and an adult predisposition to type 2
diabetes.
• Prepubertal individuals who had IUGR at birth show a greater
insulin response than prepubertal individuals who had healthy
growth as infants - increased risk of type 2 diabetes in adults who
had restriction as infants stems, instead, from increased
peripheral insulin resistance that allows the brain-sparing
physiology to occur but with a permanent reduction in skeletal-
muscle glucose transport.
• This ultimately results in beta-cell burnout.
• The causative pathophysiology is uncertain, the risk of a metabolic
syndrome in adulthood is clearly increased among individuals who
had IUGR
19.
20.
21.
22.
23.
24. • ? An association between low birth weight and adult risk of
ischemic heart disease.
• ? Adult kidney function is adversely affected by restricted
intrauterine growth.
• ? Mental health problems morbidity academic impairment
and poorer general health impaired fetal circulation, as
demonstrated by Doppler studies, in association with IUGR
results in worsened cognitive function in adulthood.
25. DETECTION OF INTRAUTERINE GROWTH
RESTRICTION
• Diagnosis by maternal physical examination - inaccurate 50%
of cases.
• A single fundaI height measurement at 32-34 weeks' -65-
85% sensitive and 96% specific for detecting the growth-
restricted foetus.
• When IUGR is suspected by maternal fundaI height,
ultrasound for estimated foetal weight (EFW) assessment
should be performed.
26. Diagnosis and Surveillance
Criteria for diagnosis of IUGR
• An EFW at or below the 10th percentile is used to identify
fetuses at risk. (Short maternal or paternal height, the
neonate's ability to maintain growth along a standardized
curve, and a lack of other signs of uteroplacental
insufficiency (eg, oligohydramnios, abnormal doppler
findings) can be reassuring)
• USG -an initial scan may be obtained in the middle of the
second trimester (at 18-20 weeks) to confirm dates, evaluate
for anomalies, and identify multiple gestations. A repeat
scan may be scheduled at 28-32 weeks' gestation to assess
fetal growth, evidence of asymmetry, and stigmata of brain-
sparing physiology (eg, oligohydramnios, abnormal doppler
findings).
27. • If the EFW is below the 10th centile, further sonographic
evaluation should be performed, including Doppler flow
studies, amniotic fluid assessment, and evaluation for
structural abnormalities.
• During initial evaluation, it is important to note whether
growth restriction is symmetric, asymmetric, or a mixed
pattern.
• Intrinsic insults occurring early in pregnancy result in a
symmetric growth restriction.
• Extrinsic insults occurring later in pregnancy will likely result
in asymmetric growth restriction.
• Every tool must be used to identify the aetiology of IUGR.
28.
29. THERAUPTIC OPTIONS
• First, behavioral strategies to quit smoking result in a lower
rate of low birth weight in babies at term among mothers
who smoke.
• Second, balanced nutritional supplements in
undernourished women and magnesium and folate
supplementation (in some studies) decrease the rate of SGA
newborns.
• Third, if malaria is the etiologic agent, maternal treatment of
malaria can increase fetal growth.
30. The administration of steroids
• The only intervention that has been shown to decrease neonatal
morbidity and mortality is the administration of steroids to
premature fetuses when delivery is anticipated.
• Odds ratio reduction with steroids, from Bernstein et al, is as
follows [7] :
• Relative risk of death, 0.54; 95% CI, 0.48-0.62
• Relative risk of respiratory distress syndrome, 0.51; 95% CI, 0.44-
0.58
• Relative risk of intraventricular hemorrhage, 0.67; 95% CI, 0.61-
0.73
• Relative risk of severe intravascular hemorrhage, 0.5; 95% CI,
0.43-0.57
• Relative risk of necrotizing enterocolitis, no difference noted
31. The IUGR fetuses can be grouped as follows:
• Small for gestational age (SGA): Small foetuses with no
discernible pathology and with normal umbilical artery and
middle cerebral artery Doppler results.
• Growth restriction: Small foetuses with recognisable
pathology/abnormal Doppler studies.
• Idiopathic growth restriction: Small foetuses with no
identifiable pathology/ abnormal Doppler studies.
32. STAGING SYSTEM
• Staging of IUGR based on foetal biometry, Doppler
cardiovascular changes, amniotic fluid volume, and clinical
parameters. In addition, the staging system is applicable to
pregnancies at any gestational age. The staging system is as
follows:
• Stage 0: Foetuses with EFW or an AC <10th percentile.
Normal Doppler of the umbilical artery and middle cerebral
artery.
• Stage I: Foetuses whose EFW or AC is <10th percentile plus
abnormal Dopplor flow of the umbilical artery or middle
cerebral artery.
33. • Stage II: Foetuses whose EFW or AC is <10th percentile plus
absent or reversed
• Doppler flow of the umbilical artery.
• Stage III: Fetuses whose EFW or AC is <10th percentile plus
absent or reverend
• Doppler flow of the ductus venosus.
• Based on the amniotic fluid index (AFI), each IUGR foetus
will be either (AFI <5 cm) or B (AFI 25 cm).
34. SITUATION-WISE MANAGEMENT
• Situation 1
• Test results – AC less than fifth percentile, low AC growth
rate, high ratio of head circumference to AC; BPS greater
than or equal to 8 and AFV normal; abnormal UV and/or
cerebroplacental ratio; normal MCA.
• Interpretation – IUGR diagnosed, asphyxia extremely rare,
increased risk of intrapartum distress.
• Recommended management – Intervention for obstetric or
maternal factors only, weekly BPS, multivessel Doppler
every 2 weeks.
35. STAGING SYSTEM AND MANAGEMENT
• Stage 0: SGA foetuses have a good prognosis ,
• managed as outpatient with dietary supplementation (NO
donors, arginine granules, Protein supplementation) and
• Doppler assessment every 2 weeks.
• If the Doppler Teams normal, delivery at term.
• If the Doppler becomes abnormal, these fetuses are
managed as Stage I IUGR fetuses.
36. • Situation 2
• See the list below:
• Test results – IUGR criteria met, BPS greater than or
equal to 8, AFV normal, UA with absent or reversed
end-diastolic velocities, decreased MCA.
• Interpretation – IUGR with brain sparing, hypoxemia
possible and asphyxia rare, at risk for intrapartum
distress.
• Recommended management – Intervention for
obstetric or maternal factors only; BPS 3 times a
week; weekly UA, MCA, and venous Doppler.
SITUATION-WISE MANAGEMENT
37. • Stage 1: Fetuses having mild IUGR, affected mothers
without pre-eclampsia are usually managed as outpatients.
• Antenatal corticosteroids
• In these fetuses - twice-weekly antenatal testing
• If the non-stress testing (NST) remains reactive and the AFI
remains >5 cm - delivery at 37 weeks' gestation.
• If the umbilical artery Doppler becomes absent/reversed -
manage as Stage II IUGR.
STAGING SYSTEM AND MANAGEMENT
38. • Situation 3
• See the list below:
• Test results – IUGR with low MCA PI; oligohydramnios; BPS
greater than or equal to 6; normal IVC, DV, and UV flow.
• Interpretation – IUGR with significant brain sparing, onset of
fetal compromise, hypoxemia common, acidemia/asphyxia
possible.
• Recommended management – If at more than 34 weeks'
gestation, deliver (route determined by obstetric factors). If
at less than 34 weeks' gestation, administer steroids to
achieve lung maturity and repeat all testing in 24 hours
SITUATION-WISE MANAGEMENT
39. • Stage II: IUGR fetuses managed as inpatients.
• During hospital management - twice-daily NST and daily
biophysical profile (BPP).
• If the NST reassuring and the BPP score between 6 and 8 -
continuation of expectant management &
• Antenatal corticosteroids at 28 weeks.
• Delivery at 34 weeks.
• If NSTs become non- reassuring or if the BPP score is <4/8 on
2 occasions at least 4 hours apart - immediate delivery By
Caesarean delivery because fetuses with an
absent/reversed flow of the umbilical artery may not
tolerate labor induction.
STAGING SYSTEM AND MANAGEMENT
40. • Situation 4
• See the list below:
• Test results – IUGR with brain sparing, oligohydramnios, BPS
greater than or equal to 6, increased IVC and DV indices, UV flow
normal.
• Interpretation – IUGR with brain sparing, proven fetal
compromise, hypoxemia common, acidemia/asphyxia likely.
• Recommended management – If at more than 34 weeks'
gestation, deliver (route determined by obstetric factors and
oxytocin challenge test [OCT] results). If at less than 34 weeks'
gestation, individualize treatment with admission, continuous
cardiotocography, steroids, maternal oxygen, and/or
amnioinfusion and then repeat all testing up to 3 times a day
depending on status.
SITUATION-WISE MANAGEMENT
41. • Stage III: IUGR fetuses are managed the same as stage II
except for delivery at 32 weeks' gestation, regardless of
gestational age at time of diagnosis.
• As with stage I and II - antenatal corticosteroids
The advantage of the above scoring system is its simplicity.
Only foetal biometry. Doppler evaluation, and the amniotic
fluid index are needed.
STAGING SYSTEM AND MANAGEMENT
42. • Situation 5
• See the list below:
• Test results – IUGR with accelerating compromise, BPS less
than or equal to 6, abnormal IVC and DV indices, pulsatile
UV flow
• Interpretation – IUGR with decompensation, cardiovascular
instability, hypoxemia certain, acidemia/asphyxia common,
high perinatal mortality, death imminent
• Recommended management – If fetus is considered viable
by size, deliver as soon as possible at tertiary center. Route
determined by obstetric factors and OCT results. Fetus
requires highest level of neonatal ICU care.
SITUATION-WISE MANAGEMENT
43. • If the umbilical artery and middle cerebral artery Doppler
are normal, Doppler study of the ductus venosus is
unnecessary because it will be normal as well.
• The presence MGR in the setting of pre-eclampsia should
not deter standard management of pre-eclampsia.
STAGING SYSTEM AND MANAGEMENT
44. • The diagnosis of severe IUGR before 32 weeks' gestation is
associated with a poor prognosis, and therapy must be
highly individualized.
• Once a decision has been made to effect delivery, the mode
of delivery is governed by evidence of acidemia, gestational
age, and Bishop score.
• Cesarean delivery without a trial of labor may be
appropriate (1) in the presence of evidence of fetal distress
by nonstress testing or reversed diastolic flow or (2) for
traditional obstetrical indications for cesarean delivery (ie,
malpresentation, prior cesarean delivery).
45. IMPORTANT CAUSES OF IUGR AND THEIR
MANAGEMENT
• The most important factor -when to deliver an IUGR fetus.
• Repeat the investigations according to the extent IUGR and
• Close monitoring is absolutely essential on a case-to-case
basis and to delay delivery as close to fetal maturity as
possible.
• Gestational diabetes mellitus and the degree of glucose
intolerance has to be identified during pregnancy. A
diagnostic 75 g oral glucose tolerance test (OGTT) after
overnight fast at least 8 hours should be tested at 24-28
weeks and must be repeated periodically to monitor glucose
control.
46. • Patients with (GDM) must be taught the importance of self
glucose monitoring (capillary).
• Pre-pregnancy counselling and
• Antenatal management are essential for optimising of
glycaemic control, keeping glycosylated hemoglobin (HbA1C)
less than 6.5-7%.
• Dietary control, oral hypoglycaemic agents or properly
chosen insulin and its dosage along with frequent
monitoring -optimum results.
• Try to prevent every complication of diabetes.
47. DIAGNOSIS
• Diagnose - Abnormalities affecting the structure and
function of the foetus as early as possible.
• Screening methods for chromosomal abnormalities have
improved over years, e.g. biochemical markers in 1 st and
2nd trimester of pregnancy,
• Advances in ultrasonography, colour Doppler and 3D and 4D
screening for birth defects;
• Invasive tests such as amniocentesis, CVS, cordocentesis for
foetal cord blood sampling
48. • Noninvasive prenatal foetal chromosomal study from
maternal blood is available only at some centers.
• Preimplantation genetic diagnosis is rarely utilized for
couples with high risk of transmitting an inherited condition.
• Depending on the case and type of anomaly, discontinuation
of pregnancy may be decided after counseling.
• Chronic urinary infection in pregnancy needs proper
diagnosis and long-term treatment.
49. • Overall general health of the patient and
• management of anaemia, hypothyroidism and infections
• Investigate - Thromboembolic disease during pregnancy
especially when there is recurrent IUGR.
• Appropriate treatment by anti thrombotic and thrombolytic
agents such as low molecular weight heparin, aspirin,
steroids are given almost through the pregnancy and
decision to deliver the patient depends on the results of
monitoring.
50. • Hypertension during pregnancy causes placental ischaemia with
endothelial dysfunction and IUGR.
• Chronic reduction in uteroplacental perfusion - detect by series of
tests—clinical, biochemical, sonographic and Doppler
• Management with antihypertensive agents, nitric oxide donors, L-
arginine treatment, low-dose aspirin - effective along with very
close monitoring timely treatment and delivery.
• Endothelial cell dysfunction - main component of the patho
physiology of pre-eclampsia and in spite of medical treatment, the
decision for timely delivery is most important.
51. Management of twins
• Delivery depends on chorionicity, prenatal screening for
chromosomal and structural abnormalities and placental
evaluation.
• Cervical length measurements and foetal growth studies in
IUGR in twin pregnancy - most important especially in
discordant and monochorionic twins.
• A careful approach to diagnosis and management – for
better outcomes, preventing unanticipated stillbirth and
allowing appropriate timing of delivery.
52. • Integration of different testing modalities allows adjustment of
monitoring interval based on Doppler parameters and a more
precise prediction of acid-base, status based on biophysical
variables.
• The presence of a well-equipped neonatal intensive care unit
(NICU) and a well-trained neonatologist – must.
• For the obstetrician and the neonatologist - the balance of fetal
risks of continuation of pregnancy the neonatal risks after birth
that dictates the timing of delivery.
53. TIMING OF DELIVERY
• There is a temporal sequence of Doppler changes preceding
the onset of late decelerations.
• Early Doppler changes occur in all the IUGR fetuses,
• Whereas late Doppler changes occur in idiopathic IUGR and
only in a few IUGR cases diagnosed in patients with pre-
eclampsia.
• In pre eclamptic patients - the changes are unpredictable,
and can occur in a few hours, and in most cases, do not
occur because delivery is done for maternal indication.
54.
55. TIMING OF DELIVERY FOR VERY PREMATURE
GROWTH-RESTRICTED FOETUSES
• At the current time, it is not possible to identify optimal
timing of delivery in very premature IUGR fetuses.
• Mostly, the decision to deliver a growth-restricted foetus
based on abnormal antenatal testing, an abnormal BPP or
NST, or abnormal Doppler study.
• In terms of survival rate, the growth-restricted foetus
delivered at >25 and <30 weeks - most problematic.
56. • The very early IUGR foetuses are delivered in the presence
of either NST or an abnormal BPP (<4/8 confirmed at 2 hours
apart).
• Fetuses diagnosed with stage I or higher IUGR involving
abnormal Doppler studies should be monitored closely.
• Still delivery solely on the basis of abnormal Doppler studies
has not been proven beneficial and, in most cases, fetuses
with abnormal Doppler studies do well in the setting of
reassuring antenatal testing.
57. MODE OF DELIVERY FOR IUGR FOETUSES
• Data seems to support caesarean delivery for a growth-
restricted foetus when there is absent or reversed flow of
the umbilical artery because these fetuses rarely tolerate
attempts at vaginal delivery.
58. Future Directions and Prevention
• Decline in the rate of IUGR from 61.5% in the historic controls to 13.3% in
those treated with aspirin and dipyridamole.
• A small decrease in the rate of preeclampsia but not IUGR (at the risk of
increased chance of abruption)
• using 150 mg of aspirin in pregnant women with abnormal UA Doppler
findings. (increase in birth weight and an increase in placental weight.)
• Beginning 100-150 mg/d of aspirin at less than 17 weeks' gestation
decreased the rate of IUGR by approximately 65% and the rate of
perinatal mortality by approximately 60%.
• Despite the theoretical benefit of aspirin in many studies, the role of
aspirin, if any, in the prevention of IUGR is still unclear.
59. SUMMARY
• Intrauterine growth restriction (IUGR) secondary to placental
insufficiency - a major cause of perinatal morbidity and
mortality worldwide.
• No single test that appears superior to the other available
tests for determining the timing of delivery of the growth-
restricted fetus.
• The presence of a well trained neonatologist at the time of
delivery - valuable.
• A few days gained by the foetus in utero between 25 weeks
and 30 weeks gestation, can make a difference in the future
of the IUGR baby.