
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Dyspareunia and Vulvodynia Treatment Guide
Similar to Dyspareunia and Vulvodynia Treatment Guide (20)
More from alka mukherjee
More from alka mukherjee (20)
Recently uploaded
Recently uploaded (20)
Dyspareunia and Vulvodynia Treatment Guide
- 1. DYSPAREUNIA & VULVODYNIA DR ALKA MUKHERJEE DR APURVA MUKHERJEE NAGPUR M.S. INDIA
- 2. DR ALKA MUKHERJEE MBBS DGO FICOG FICMCH PGDCR PGDMLS MA(PSY) Director & Consultant At Mukherjee Multispecialty Hospital MMC ACCREDITATED SPEAKER MMC OBSERVER MMC MAO – 01017 / 2016 Present Position Director of Mukherjee Multispecialty Hospital Hon.Secretary INTERNATIONAL COUNCIL FOR HUMAN RIGHTS Hon.Secretary NARCHI NAGPUR CHAPTER (2018-2020) Hon.Secretary AMWN (2018-2021) Hon.Secretary ISOPARB (2019-2021) Life member, IMA, NOGS, NARCHI, AMWN & Menopause Society, India, Indian medico-legal & ethics association(IMLEA), ISOPRB, HUMAN RIGHTS Founder Member of South Rapid Action Group, Nagpur. On Board of Super Specialty, GMC, IGGMC, AIIMS Nagpur, NKPSIMS, ESIS and Treasury, Nagpur for “ WOMEN SEXUAL HARASSMENT COMMITTEE.” mukherjeehospital@yahoo.com www.mukherjeehospital.com https://www.facebook.com/ Mukherjee Multispeciality https://www.instagram.com/ Achievement Winner of NOGS GOLD MEDAL – 2017-18 Winner of BEST COUPLE AWARD in Social Work - 2014 APPRECIATION Award IMA - MS Past Position Organizing joint secretary ENDO-GYN 2019 Vice President IMA Nagpur (2017-2018) Vice President of NOGS(2016-2017) Organizing joint secretary ENDO-GYN Organizing secretary AMWICON – 2019
- 3. Dyspareunia • Dyspareunia is the term for recurring pain in the genital area or within the pelvis during sexual intercourse. • The pain can be sharp or intense. It can occur before, during, or after sexual intercourse. • Dyspareunia is more common in women than men. • It has many possible causes, but it can be treated. • Complex disorder: 1. Superficial - superficial dyspareunia is pain localized to the vulva or vaginal entrance 2. Deep - deep dyspareunia is pain perceived inside the vagina or lower pelvis, which is often associated with deep penetration 3. Primary - primary dyspareunia occurs at initial intercourse, and 4. Secondary dyspareunia occurs after some time of pain-free intercourse.
- 4. Vulvodynia • Vulvodynia is a chronic pain that is defined as genital pain with no known etiology that lasts more than three months and may or may not be associated with sexual intercourse . • The International Society for the Study of Vulvovaginal Diseases (ISSVD), the International Society for the Study of Women’s Sexual Health (ISSWSH), and the International Pelvic Pain Society (IPPS) further describe vulvodynia • by the site of pain (localized, generalized, or mixed); • if it is provoked, spontaneous, or mixed; or • if the pain is intermittent, persistent, constant, immediate, or delayed • Localized vulvodynia refers to pain limited to the vulvar vestibule around the hymeneal ring at the entrance to the vagina, and • generalized vulvodynia is defined as pain affecting the entire vulvar region • Vulvodynia has no clear etiology.
- 5. ISSVD, ISSWSH, and IPPS potential associated Factors: • Other pain syndromes, • Genetics, • Hormonal factors, • Inflammation, • Musculoskeletal or neurologic mechanisms, • Psychosocial factors, and • Structural defects
- 6. Difference between Dyspareunia • Descriptive term for the symptom of pelvic or vaginal pain associated with intercourse (i.E., It describes pain that always occurs with provoking touch such as intercourse). • Dyspareunia can occur at the entrance of the vagina, deep in the vaginal canal, or in the pelvis. • Dyspareunia may be acute or chronic, • Can be used to describe pain that coexists with other comorbidities such as endometriosis, interstitial cystitis, pelvic floor myalgias, and vulvar dermatoses. vulvodynia • Vulvodynia may occur with or without provocation (i.E.,Spontaneously). • Vulvodynia is localized to the vulva and vaginal introitus. • Vulvodynia is a term used specifically for the classification of chronic pain (i.E., Pain lasting longer than three months). • Can be used to describe pain that coexists with other comorbidities such as endometriosis, interstitial cystitis, pelvic floor myalgias, and vulvar dermatoses.
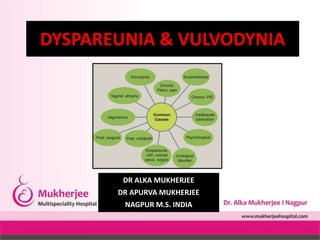
- 7. Causes • vaginal dryness from menopause, childbirth, breastfeeding, medications, or too little arousal before intercourse • skin disorders that cause ulcers, cracks, itching, or burning • infections, such as yeast or urinary tract infections (UTIs) • injury or trauma from childbirth, an accident, an episiotomy, a hysterectomy or pelvic surgery •vulvodynia, or pain centered in the vulva area •vaginitis, or inflammation of the vagina •vaginismus, or a spontaneous tightening of the muscles of the vaginal wall •endometriosis •cystitis •pelvic inflammatory disease (PID) •uterine fibroids •irritable bowel syndrome (IBS) •Radiation and chemotherapy
- 8. Factors that reduce sexual desire or affect a person’s ability to become aroused can also cause dyspareunia. • Stress, which can result in tightened muscles of the pelvic floor • Fear, guilt, or shame related to sex • Self-image or body issues • Medications such as birth control pills • Relationship problems • Conditions such as cancer, arthritis, diabetes, and thyroid disease • History of sexual abuse or rape
- 9. Symptoms • Dyspareunia pain can vary. Pain may occur: • In the vagina, urethra, or bladder • During penetration • During or after intercourse • Deep in the pelvis during intercourse • After pain-free intercourse • Only with specific partners or circumstances • With tampon use • Along with burning, itching, or aching • With a feeling of stabbing pain, similar to menstrual cramps
- 10. Who’s at risk for dyspareunia? • Both women and men can experience dyspareunia, but the condition is more common in women. Dyspareunia is one of the most common problems of postmenopausal women. • Around 75 percent of women have painful intercourse at some time, according to the American College of Obstetricians and Gynecologists (ACOG), a woman is at an increased risk if she: • Take medications that cause vaginal dryness • Have a viral or bacterial infection • Are postmenopausal
- 11. Diagnosis • A complete medical and sexual history. • Possible questions a doctor may ask: • When and where do she feel pain? • Which partners or positions cause pain? • Do any other activities cause pain? • Does her partner want to help? • Are there other conditions that may be contributing to her pain?
- 12. Vulvar anatomy Physical examination of patients with genital pain should include an external musculoskeletal evaluation, followed by external visual and sensory examination, as well as internal single digit palpation of the pelvic floor muscles. If tolerated by the patient, the provider may proceed to a bimanual examination and a speculum exam.
- 13. • The internal musculoskeletal and vaginal single-digit exam - most reliable method for evaluating pelvic muscle tenderness • Using the index finger, the examiner can palpate the lateral, anterior, and posterior walls of the vagina, the urethra, and pelvic floor muscles (levator ani, coccygeus, piriformis, and obturator internus). • Access the specific areas for tone, tenderness, or involuntary spasms of the muscles of the introitus and pelvic floor • Tenderness during minimal or moderate palpation is considered abnormal; pelvic and vaginal structures can tolerate approximately 2 kg of pressure without pain. • The patient is then asked to squeeze or contract around the single digit to assess their muscle strength. An effort should also be made to identify any scars from previous surgeries, episiotomy, or trauma.
- 16. Vaginal cotton swab examination
- 17. Important elements to discuss during clinical evaluation of female sexual pain • Medical History Questions a) PAIN CHARACTERISTICS - Timing, duration, quality, location, provoked, or unprovoked b) MUSCULOSKELETAL HISTORY Pelvic floor surgery, trauma, obstetrics c) BOWEL AND BLADDER HISTORY Constipation, diarrhea, urgency, frequency d) SEXUAL HISTORY Frequency, desire, arousal, satisfaction, relationship e) PSYCHOLOGICAL HISTORY Mood disorder, anxiety, depression f) HISTORY OF ABUSE Sexual, physical, neglect
- 18. • A pelvic examination is also common in diagnosis. A look at the external and internal pelvic area for signs of: • dryness • inflammation or infection • anatomical problems • genital warts • scarring • abnormal masses • endometriosis • tenderness • Pap test • pelvic ultrasound • culture test to check for bacteria or yeast infection • urine test • allergy test • counseling to determine the presence of emotional causes
- 19. Treatment • Antibiotics • Antifungal medicines • Topical or injectable corticosteroids • Trying alternative medications may restore natural lubrication and reduce pain. • Low estrogen levels cause dyspareunia in some women. A prescription tablet, cream, or flexible ring can deliver a small, regular dose of estrogen to the vagina.
- 20. Local Anesthetics • Sensitization of peripheral vestibular nerves has been suggested as a possible mechanism of pain in vulvodynia • topical anesthetics, such as lidocaine, can be used to relieve pain during intercourse • useful for short-term therapy and in combination with other therapies (e.g., physical therapy and botulinum toxin). • Local anesthetics are theorized to desensitize peripheral vulvar and vaginal nerves and achieve pain relief. Typically, topical 5% lidocaine is used once or twice daily with reevaluation after six to eight weeks of use
- 21. Hormonal Treatment • Vulvovaginal atrophy caused by decreased levels of estrogen is a common problem in aging women. • In patients who present with the main symptoms of atrophy, dryness, and dyspareunia, the first line of therapy consists of topical estrogen to restore normal vaginal ph levels and thicken and increase cell numbers leading to the revascularization of the epithelium • low-dose conjugated estrogens available in the forms of vaginal inserts (e.G., Cream, tablet, and ring) can be applied periodically from a few times a week to every three months. • Topical estrogen should be considered to avoid the systemic effect of oral estrogen • Patients using estrogen supplementation in any form should be followed clinically and estrogen supplementation is contraindicated in patients with certain comorbidities such as breast cancer and uncontrolled cardiovascular disease. • Topical vaginal estrogen therapy may take up to four weeks before patients notice an effect.
- 22. Anti-Inflammatory Agents • Tissue levels of interleukin-B, an inflammatory mediator cytokine, have been reported to be higher in the hymenal region of the vestibule of women with vulvodynia • Injectable anti-inflammatory agents such as corticosteroids, interferons, and mast cell stabilizers have been used to treat vulvodynia with some improvement
- 23. Botulinum Type A • Injection of botulinum toxin A into the pelvic floor muscles has been shown in some studies to decrease dyspareunia and vulvodynia caused by pelvic floor myalgia and contracture . • Botulinum toxin A is hypothesized to inhibit nociceptors leading to a decrease in peripheral and central sensitization associated with vulvodynia . • A long-term assessment of the effectiveness of botulinum injections after 24 months revealed that patients could have sexual intercourse and had improved quality of life • Not recommended as a first-line therapy as further clinical trials of botulinum type A are needed, but it is used as an adjunct to other therapies
- 24. Systemic Medications • Tricyclic antidepressants and anticonvulsants Tricyclic antidepressants – amitriptyline reduces peripheral nerve sensitization and have been used in the management of neuropathic pain - take up to three weeks to achieve pain control
- 25. Physical Therapy and Behavioral Therapy • Pelvic floor physical therapy - it allows the pelvic floor muscles to relax and retrains pain receptors. • Cognitive behavioral therapy effective in reducing the anxiety and fear related to dyspareunia • Cognitive behavioral therapy focuses on patterns of thinking and helps identify behaviors associated with negative thoughts and feelings • Non-invasive and safe therapeutic option
- 26. Home care • These home remedies can also reduce dyspareunia symptoms: • Use water-soluble lubricants. • Have sex when patient and partner are relaxed. • Communicate openly with partner about pain. • Empty the bladder before sex. • Take a warm bath before sex. • Take an over-the-counter pain reliever before sex. • Apply an ice pack to the vulva to calm burning after sex
- 27. Surgical Therapy • Last resort when all conservative and medical management options have failed or when surgery is indicated to determine and/or treat pelvic adhesions, endometriosis, or pelvic organ prolapse. • The surgical options are specific to the disorder: 1. Vulvar vestibulectomy, 2. Lysis of pelvic adhesions, or 3. Excision of endometriosis • Thorough counseling is necessary prior to pursuing surgical treatment. • Patients must understand that surgery may improve their pain, and their pain may sometimes return or worsen. • Vestibulectomy can be an effective treatment only for localized, provoked vestibulodynia - significant pain relief in 60% to 90% of patients • Generally, surgical techniques include a complete vulvar vestibulectomy, which involves excision of the mucosa of the entire vulvar vestibule and the mucosa adjacent to the urethra, or a modified vestibulectomy, which limits the excision of mucosa to the posterior vestibule .
- 28. Preventing dyspareunia • To reduce the risk of pain during intercourse: • After childbirth, wait at least six weeks before resuming sexual intercourse. • Use a water-soluble lubricant when vaginal dryness is an issue. • Use proper hygiene. • Get proper routine medical care. • Prevent sexually transmitted diseases (stds) by using condoms or other barriers. • Encourage natural vaginal lubrication with enough time for foreplay and stimulation.
- 29. SUM-UP • Despite the prevalence and impact of dyspareunia, many women do not seek care. • Women with dyspareunia often suffer in silence and feel that their pain has not been assessed or validated by providers. • Dyspareunia and vulvodynia can be challenging to diagnose and may require a multidisciplinary approach; therefore, a comprehensive and systematic exam is required to understand the specific causes of genital pain. • Treatments often involve multimodal approaches that include education, medication, cognitive behavioral therapy, physical therapy, and possibly surgery.