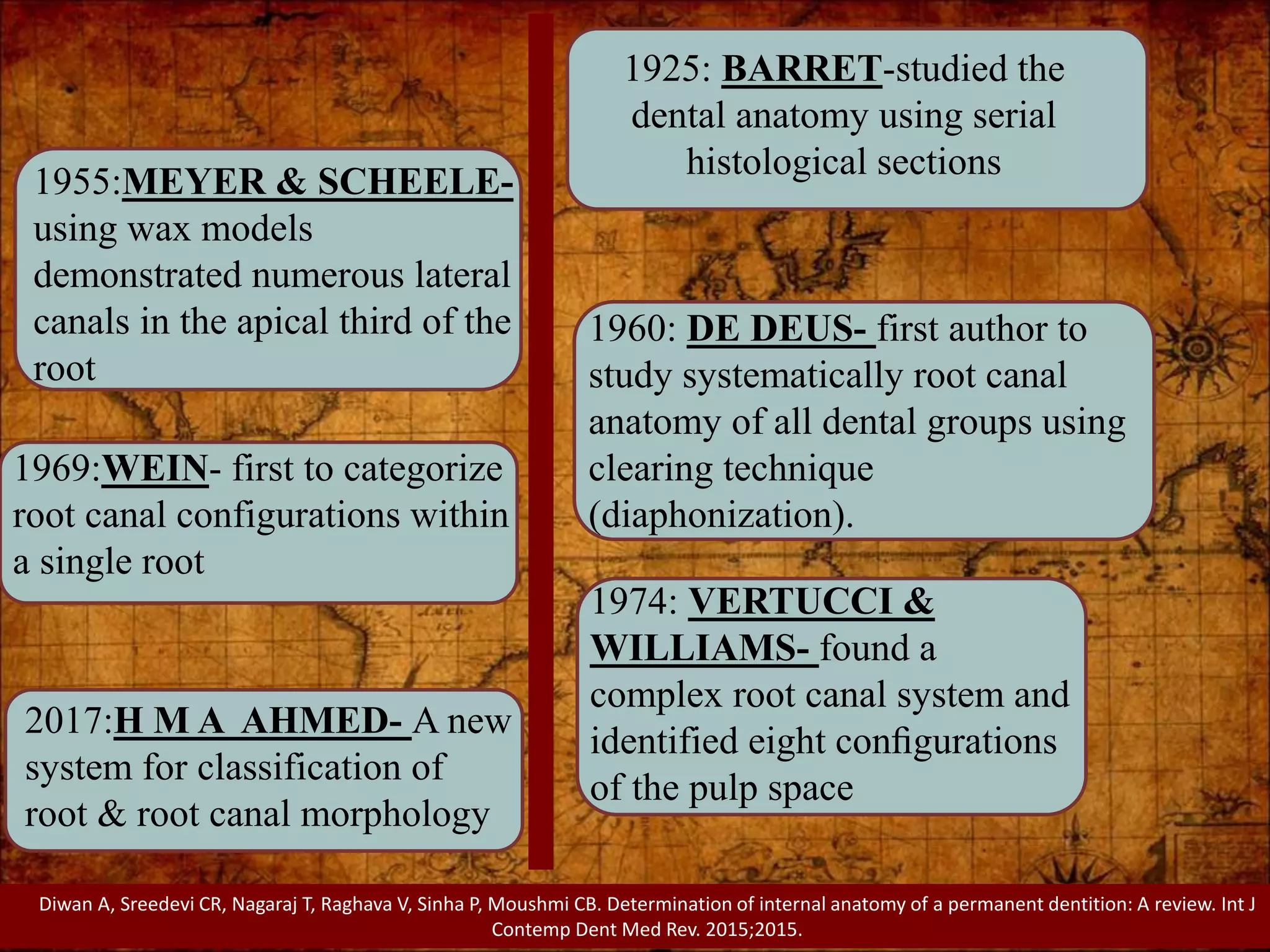
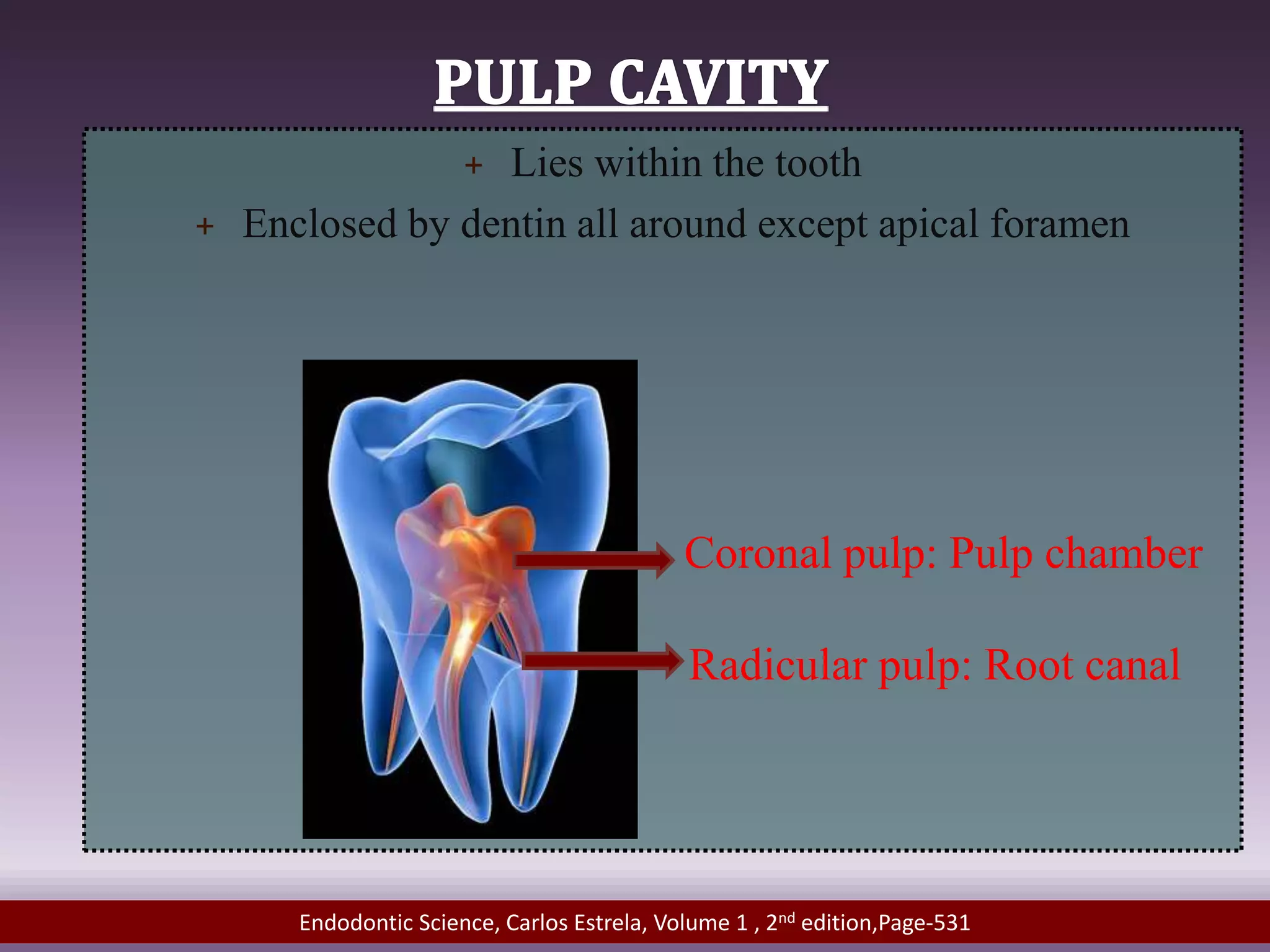
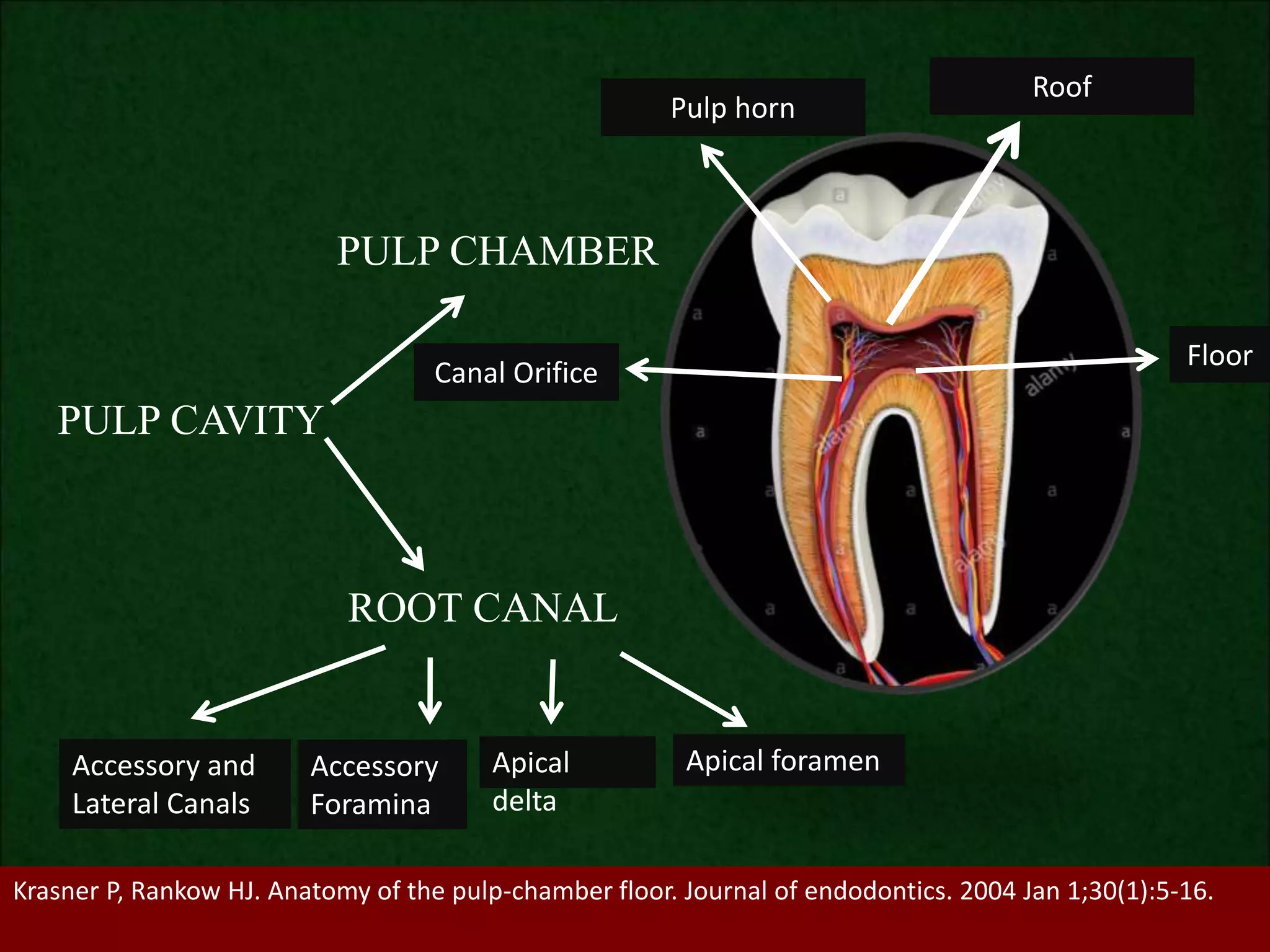
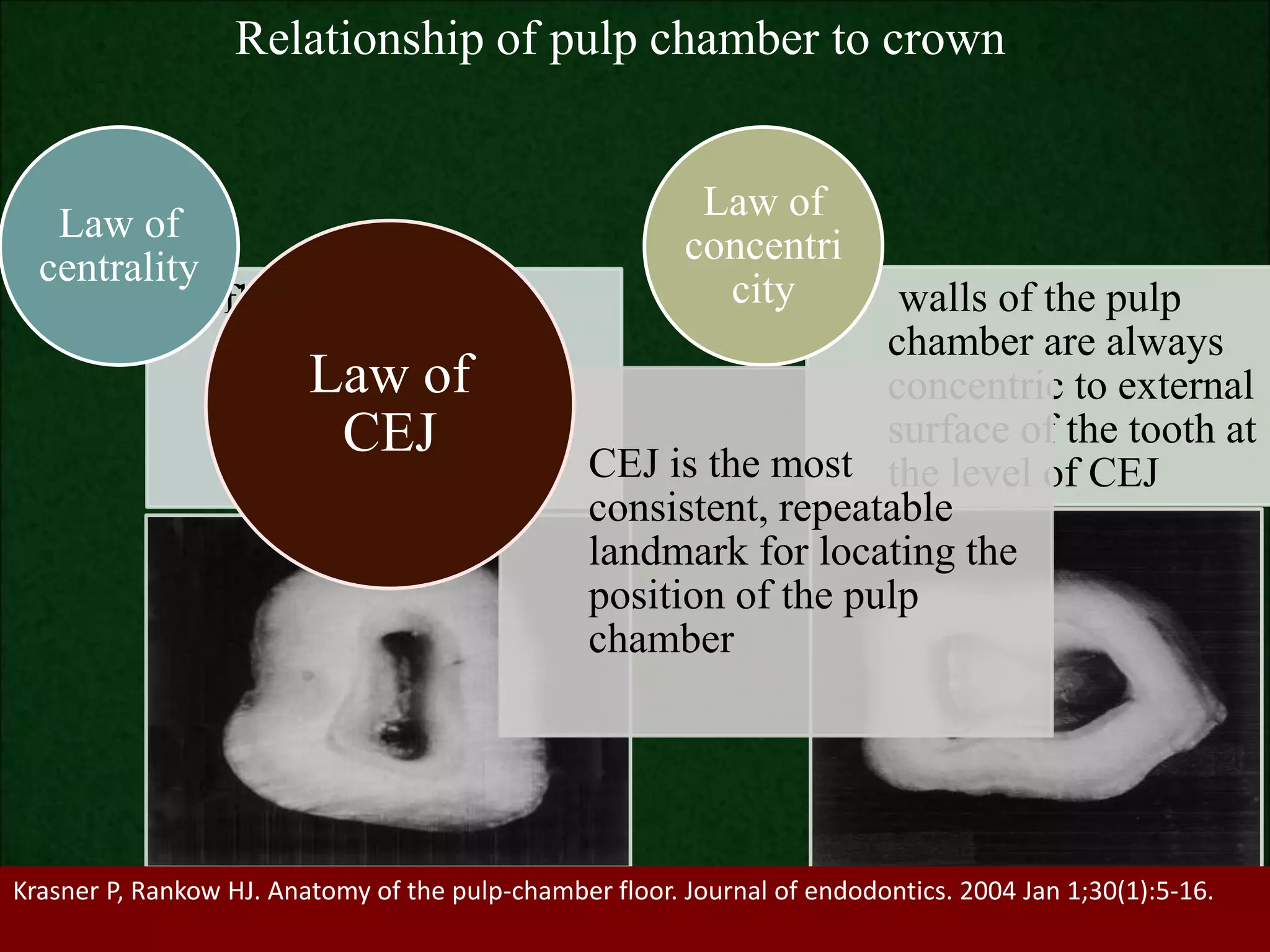
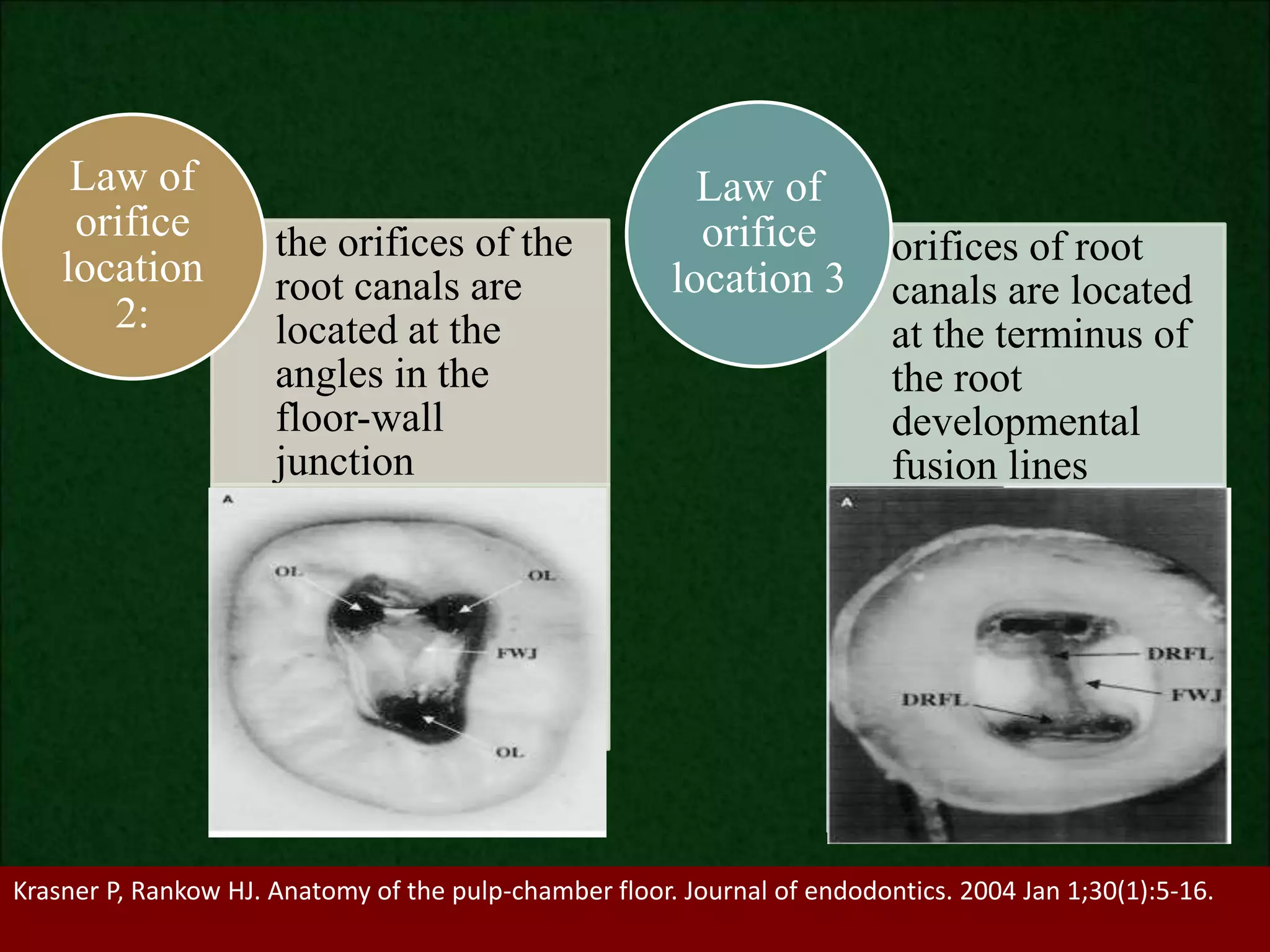
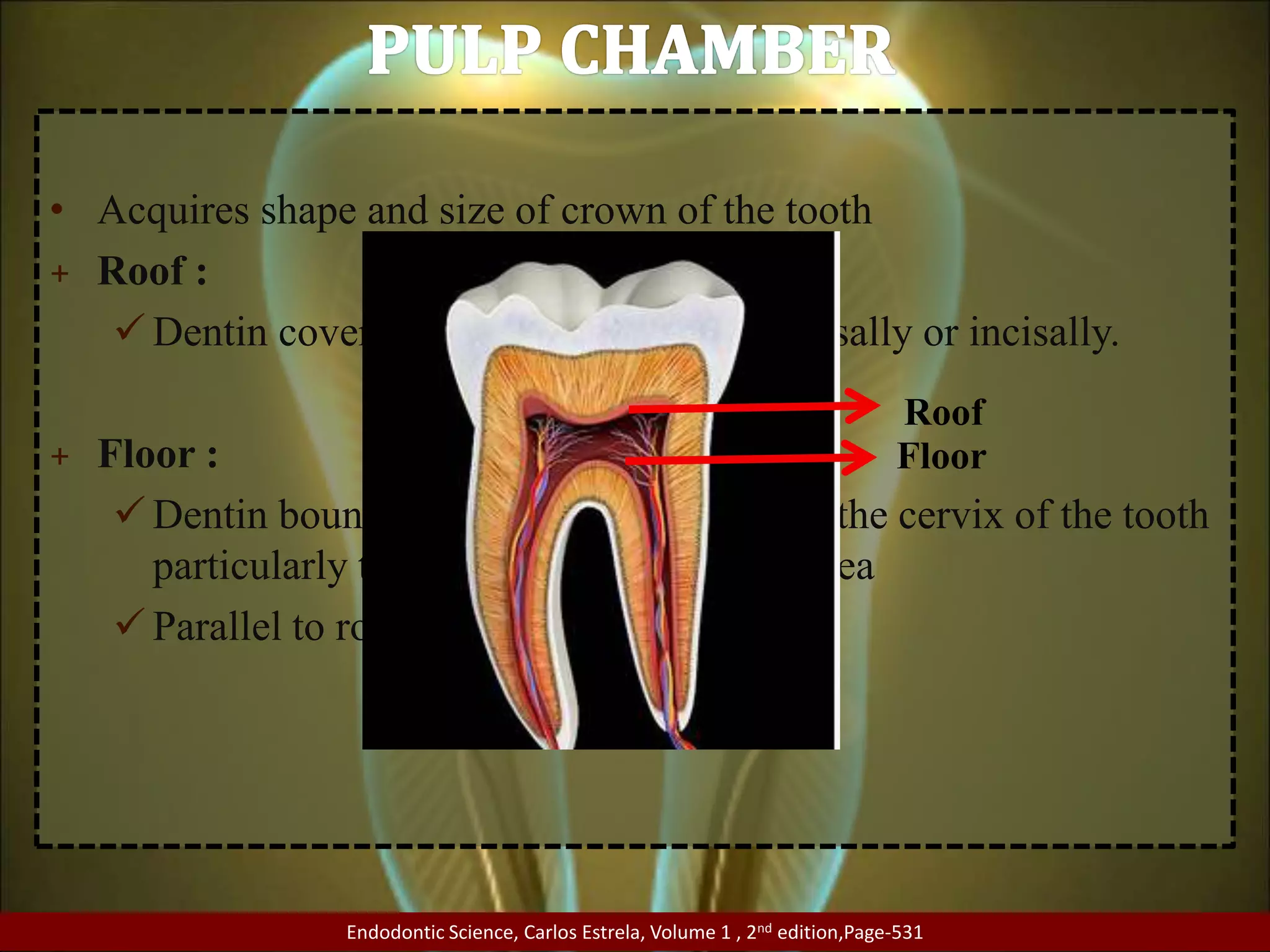
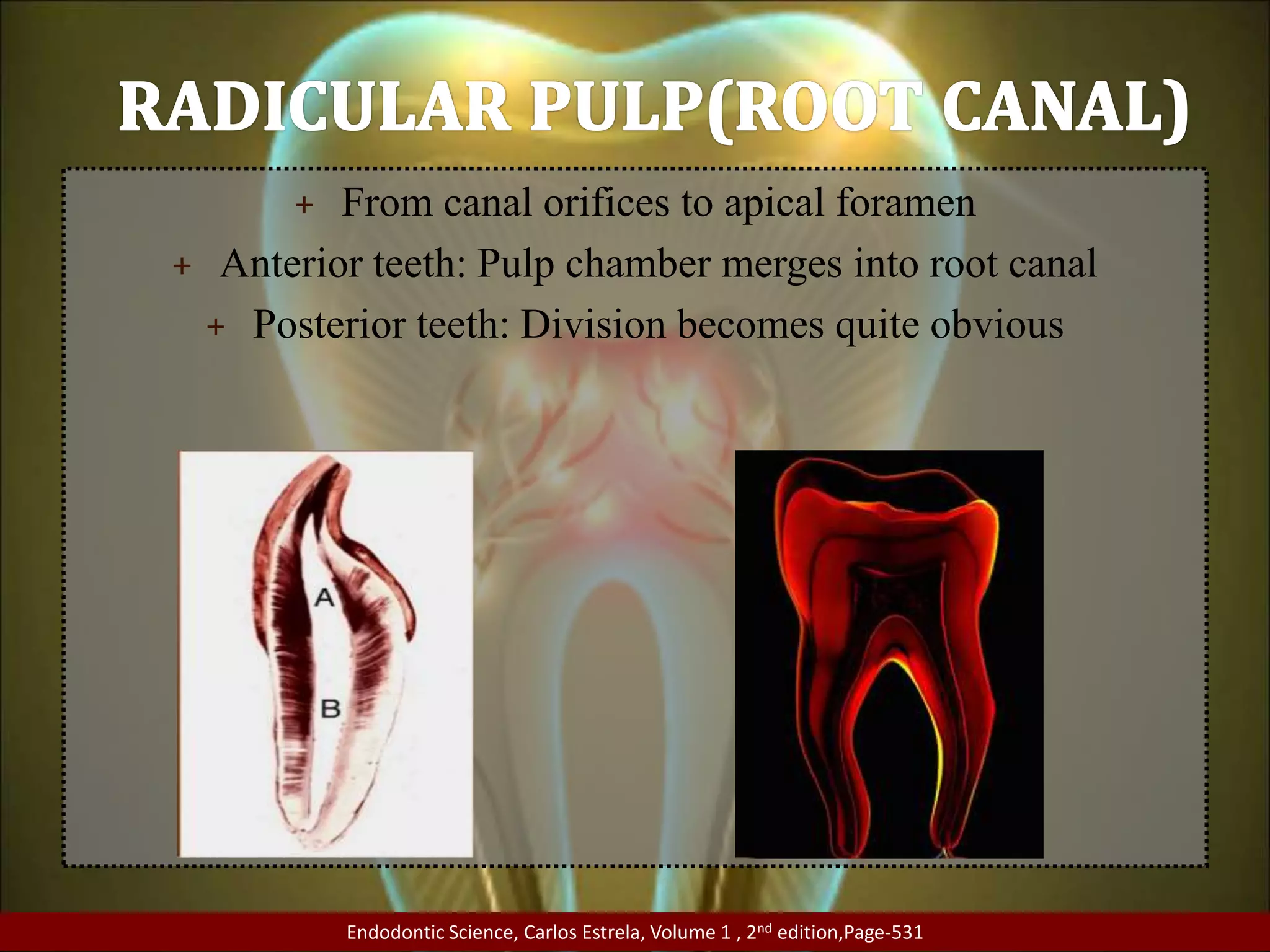
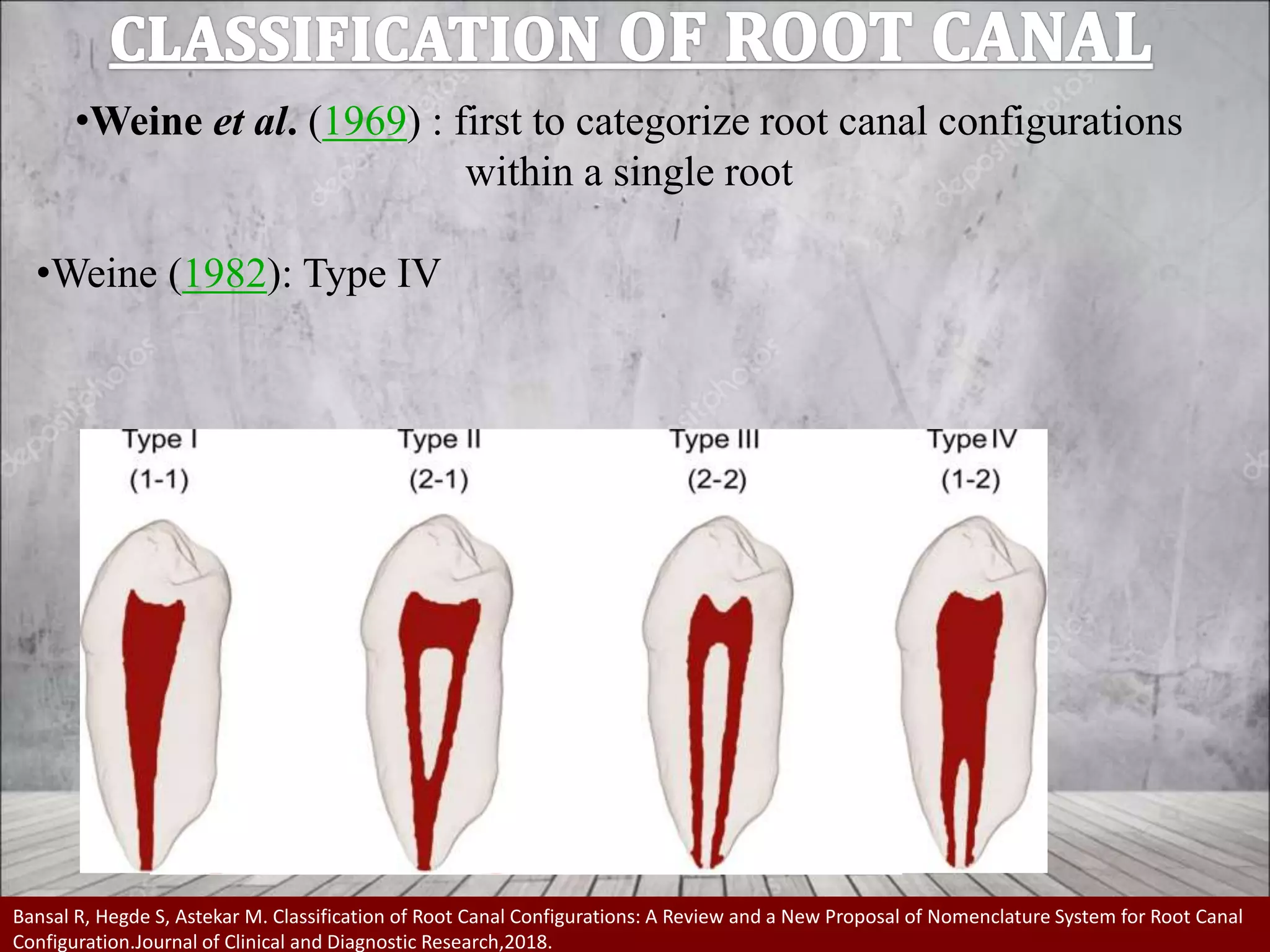
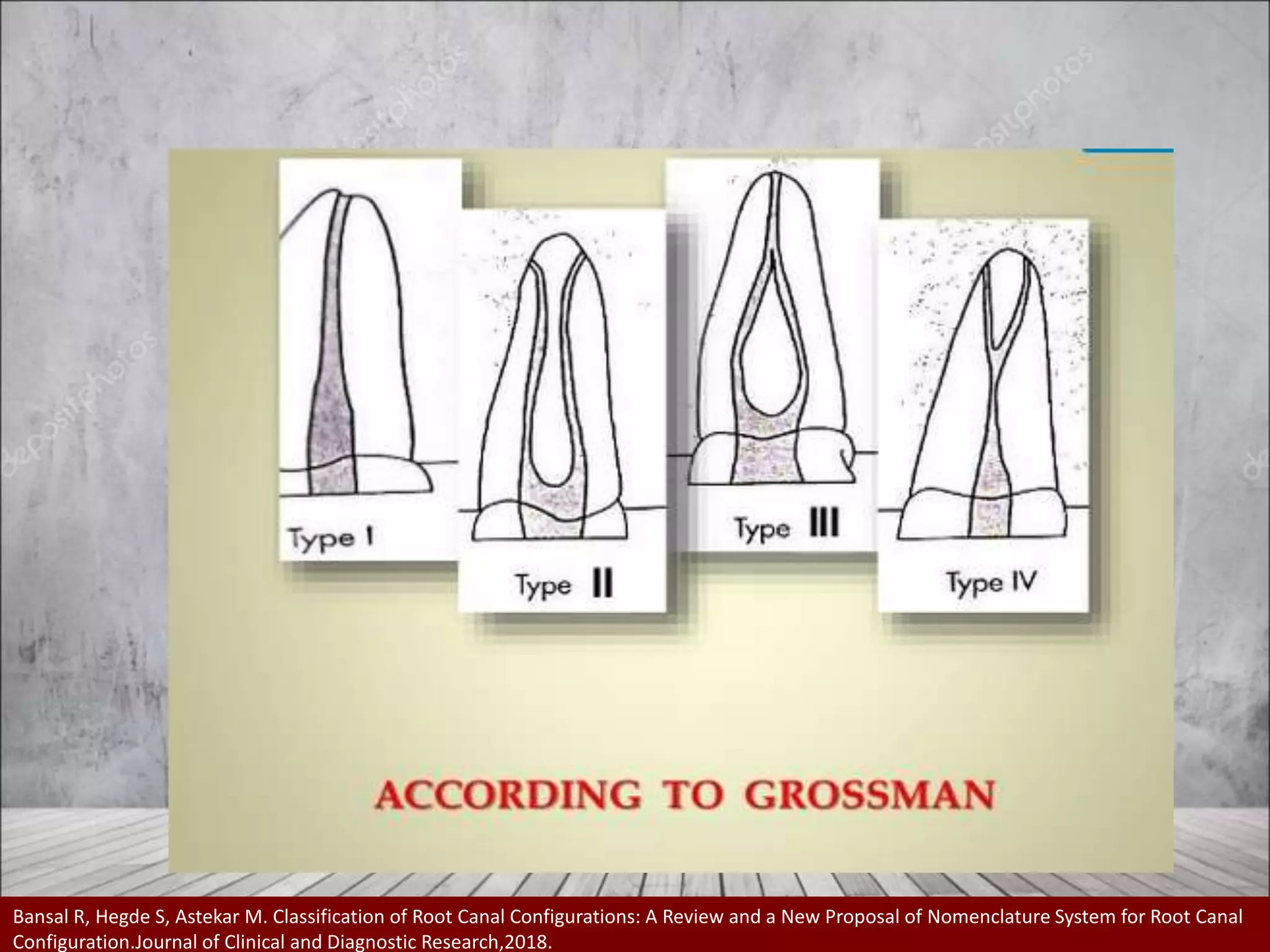
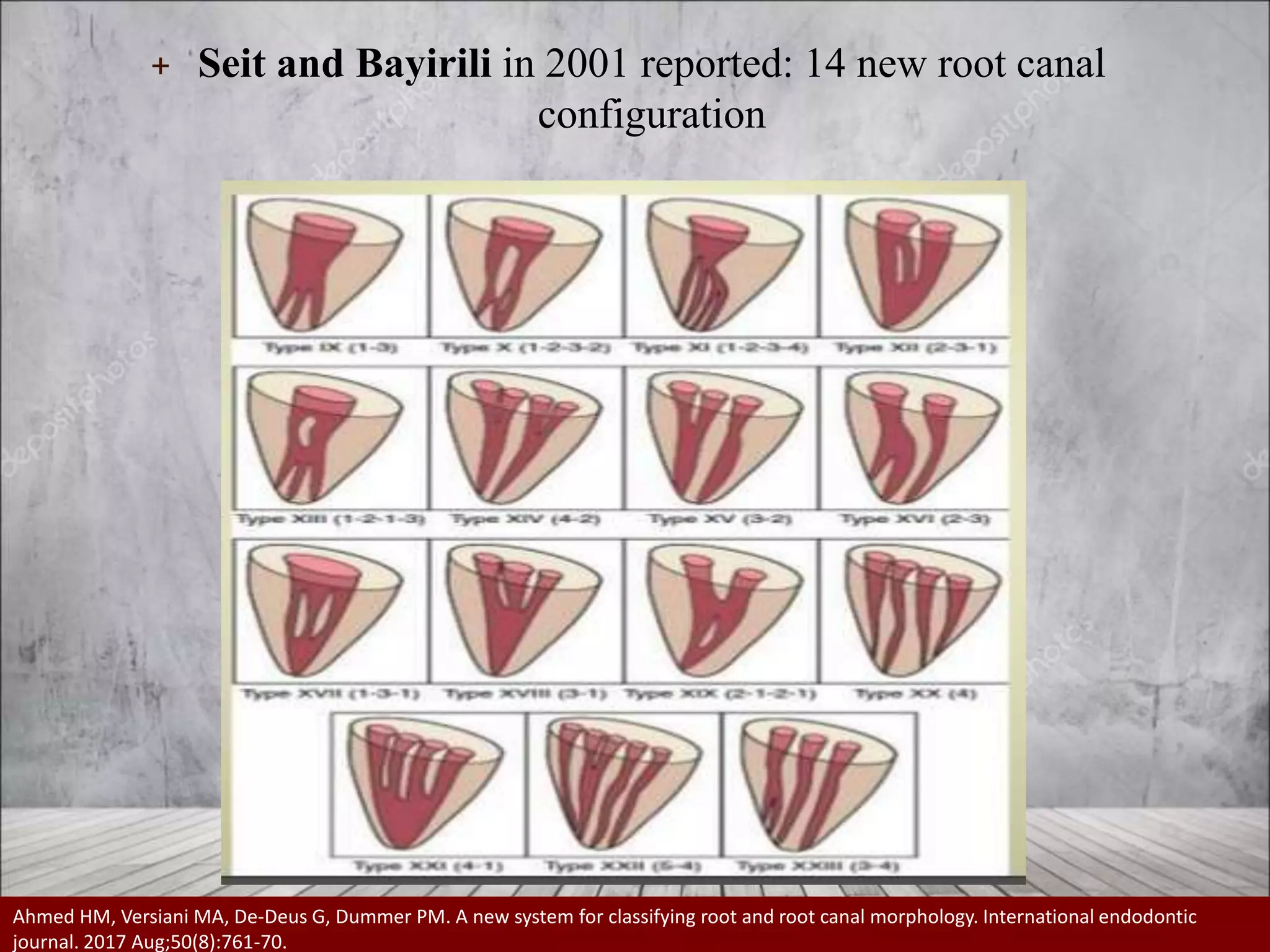
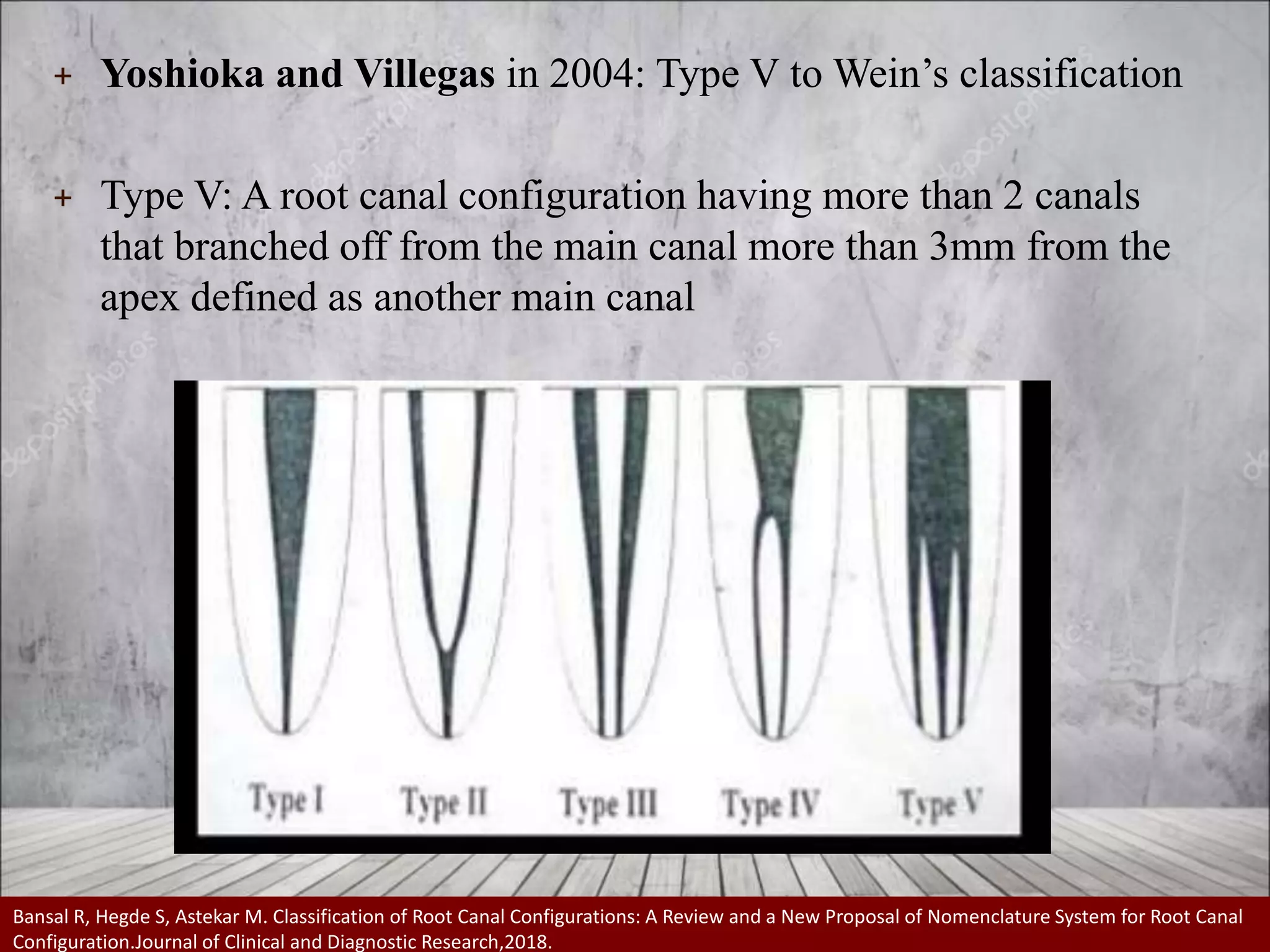
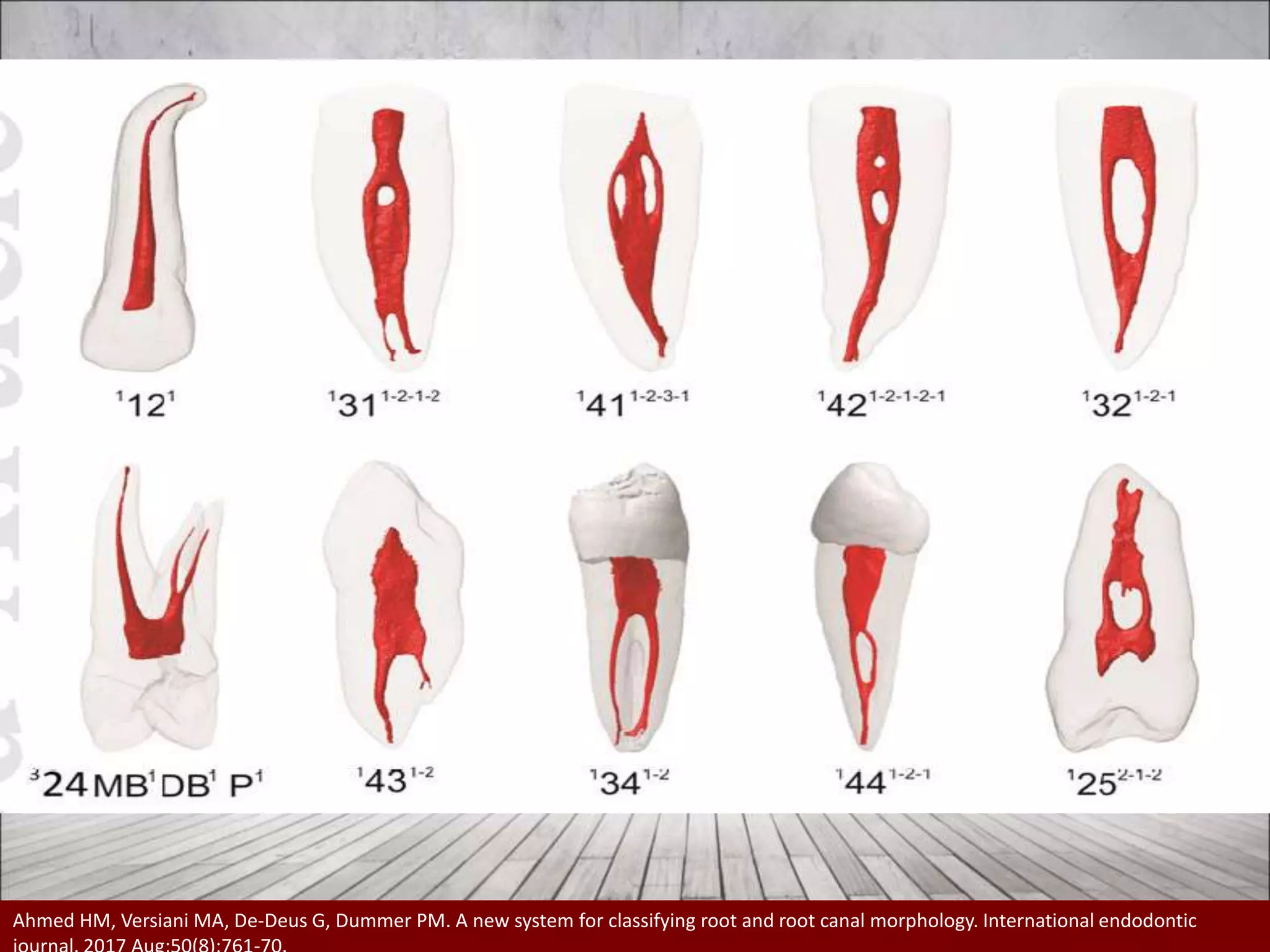
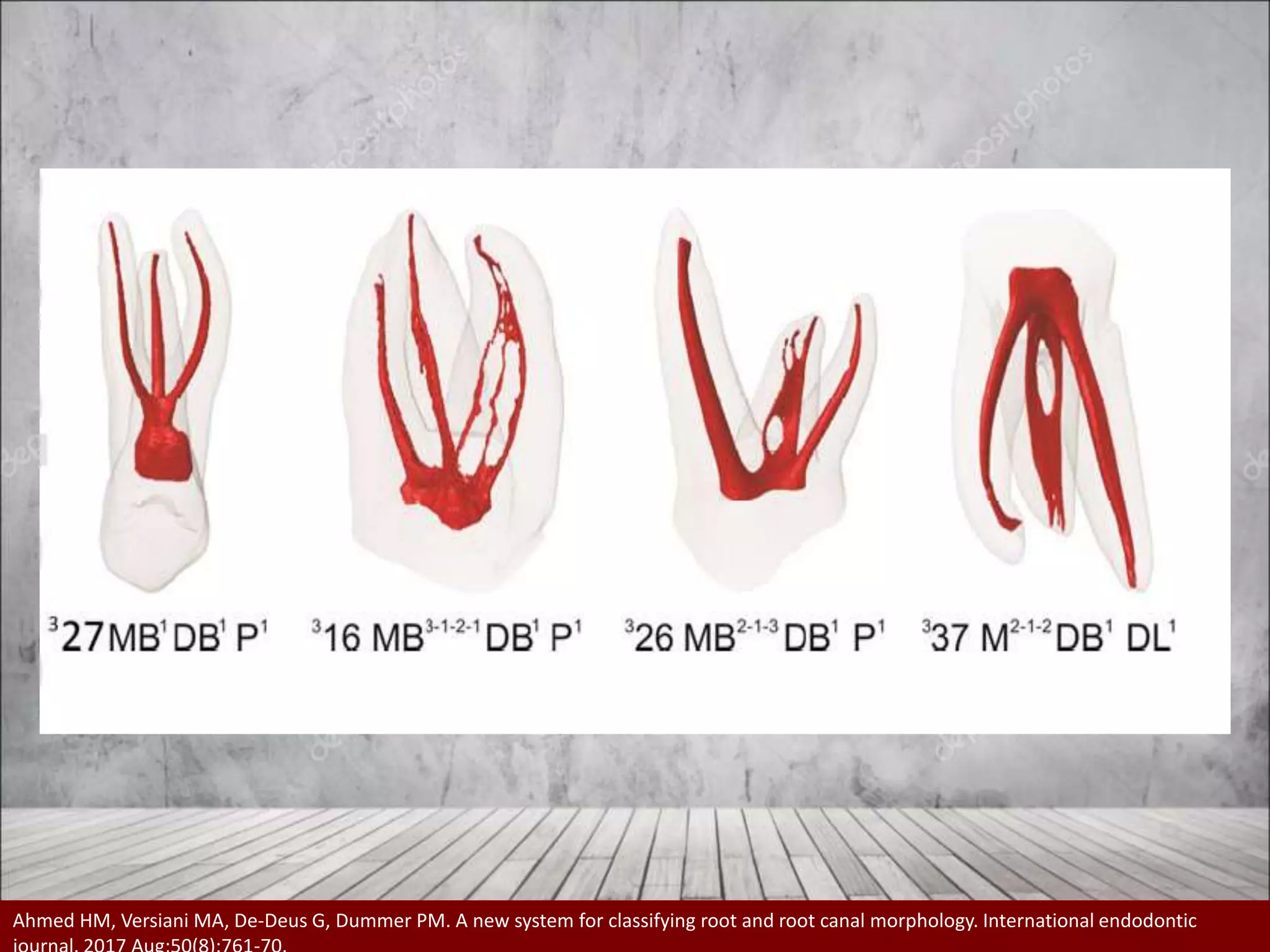
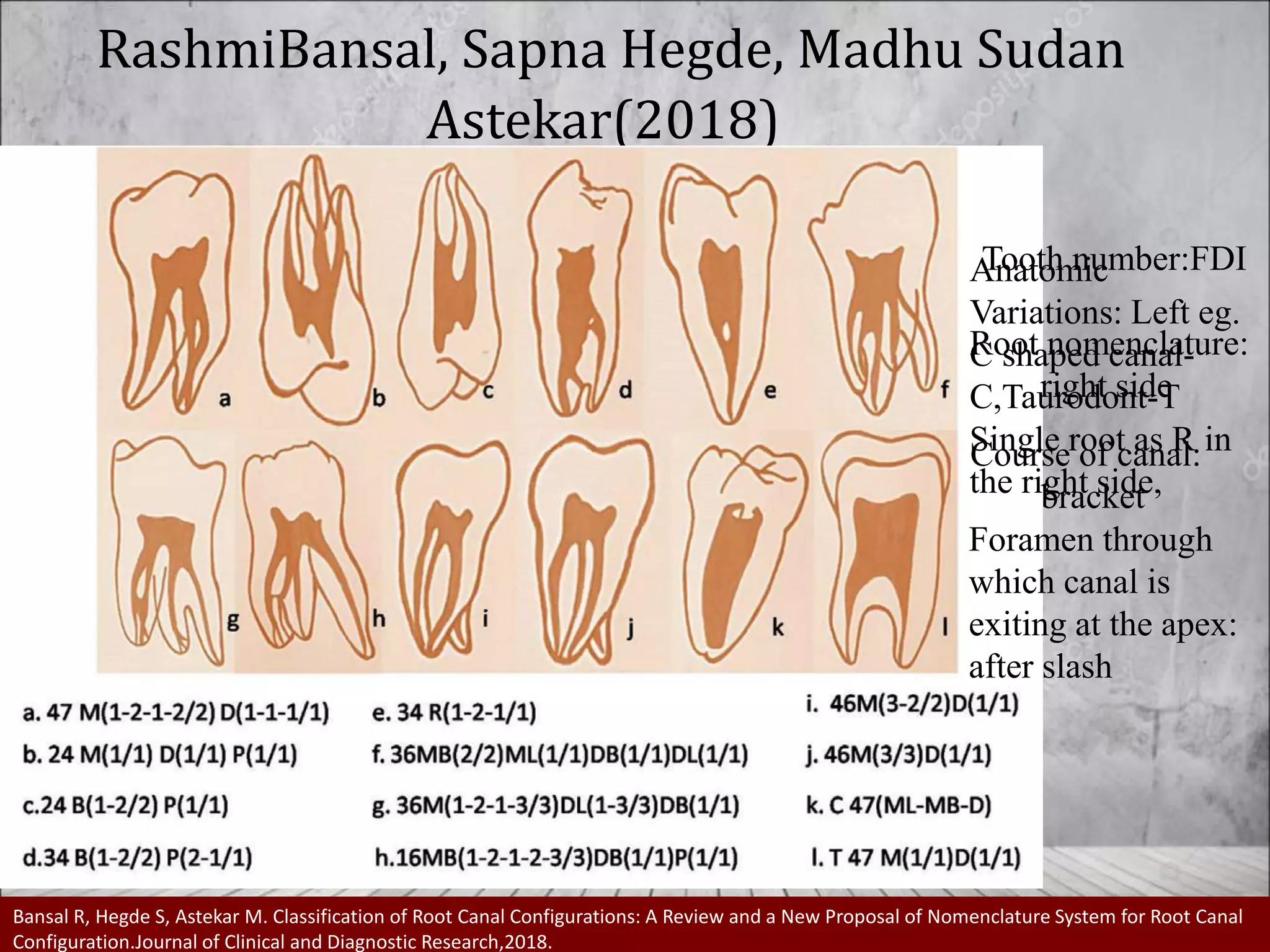
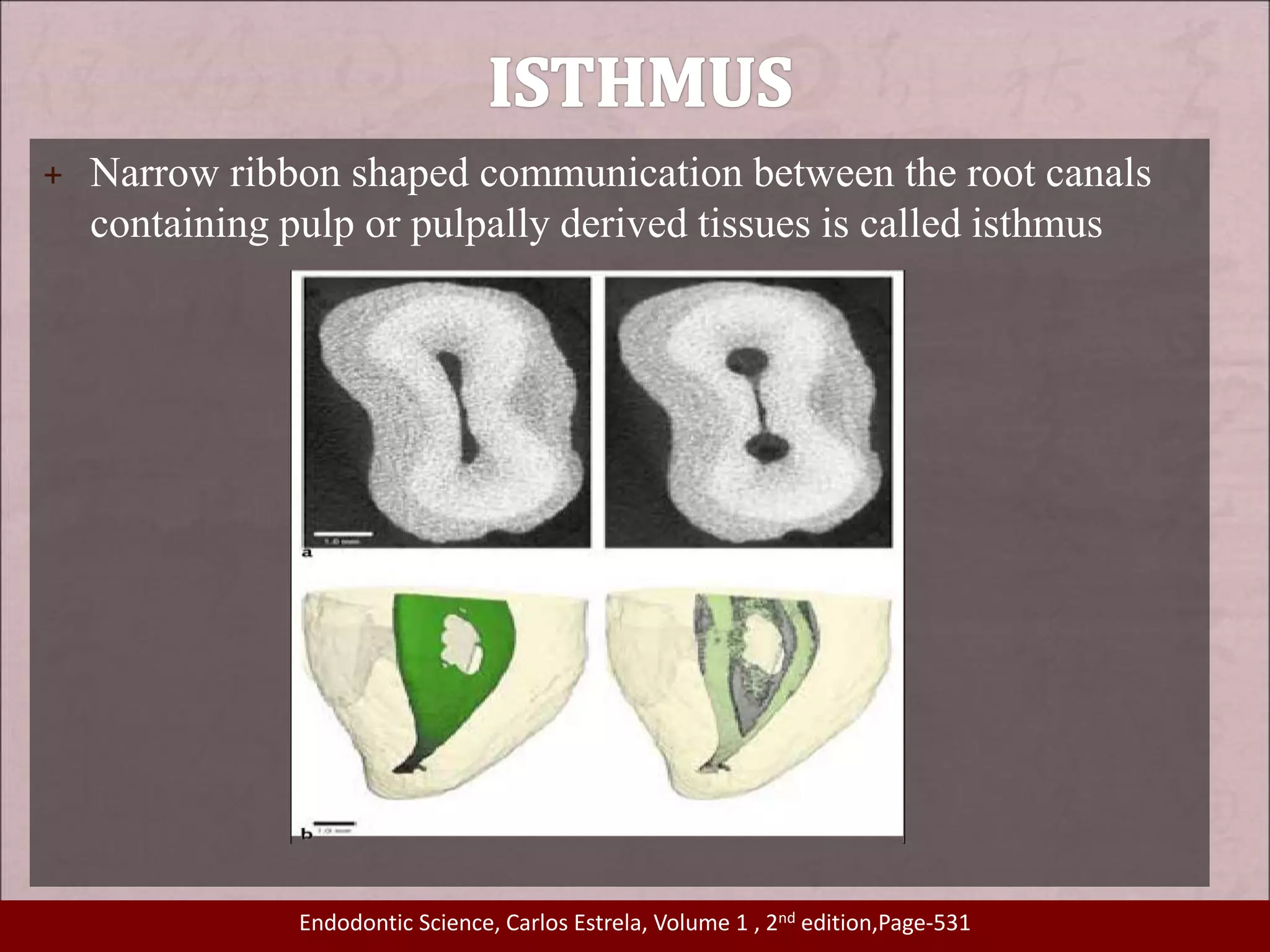
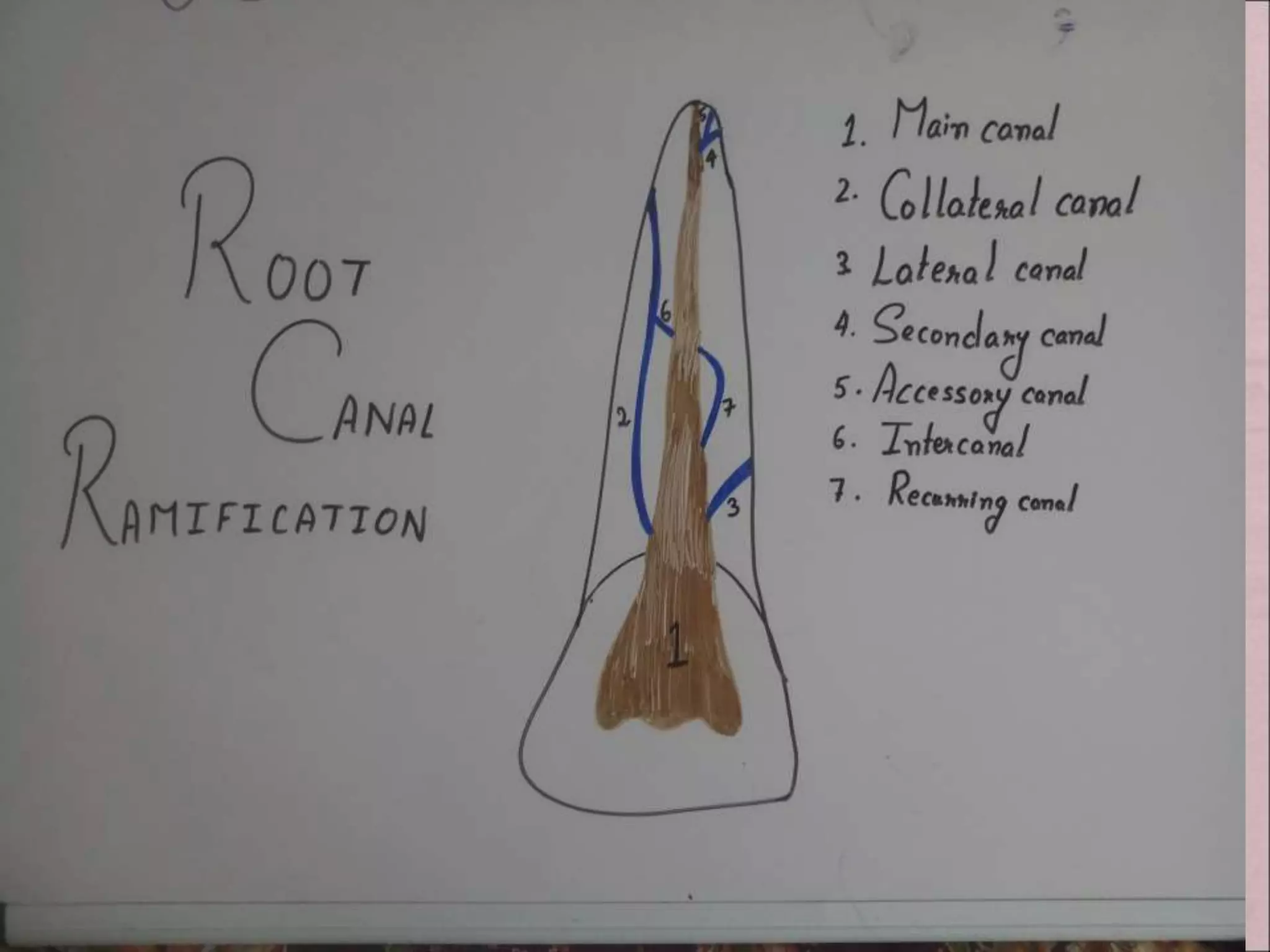
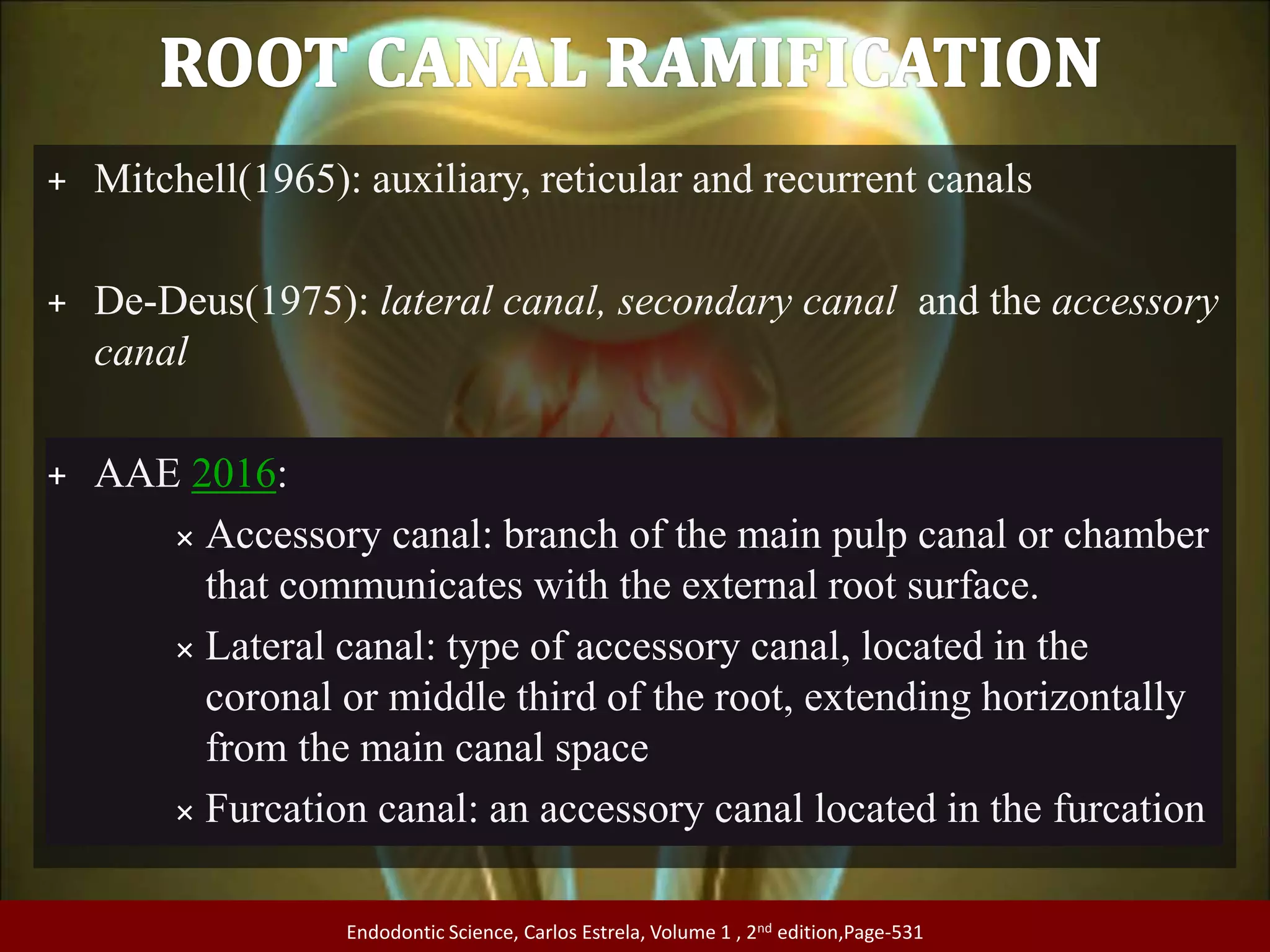
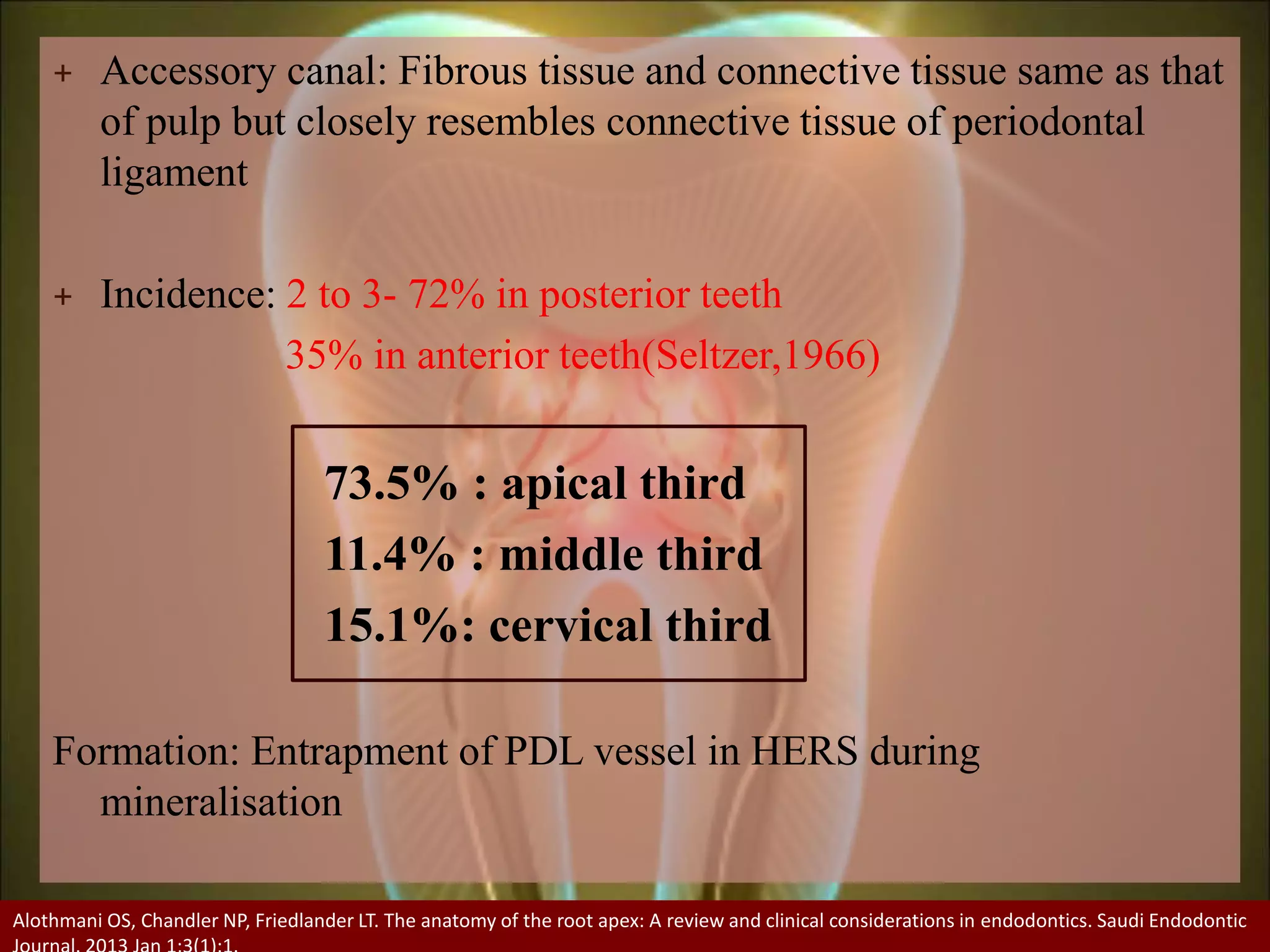
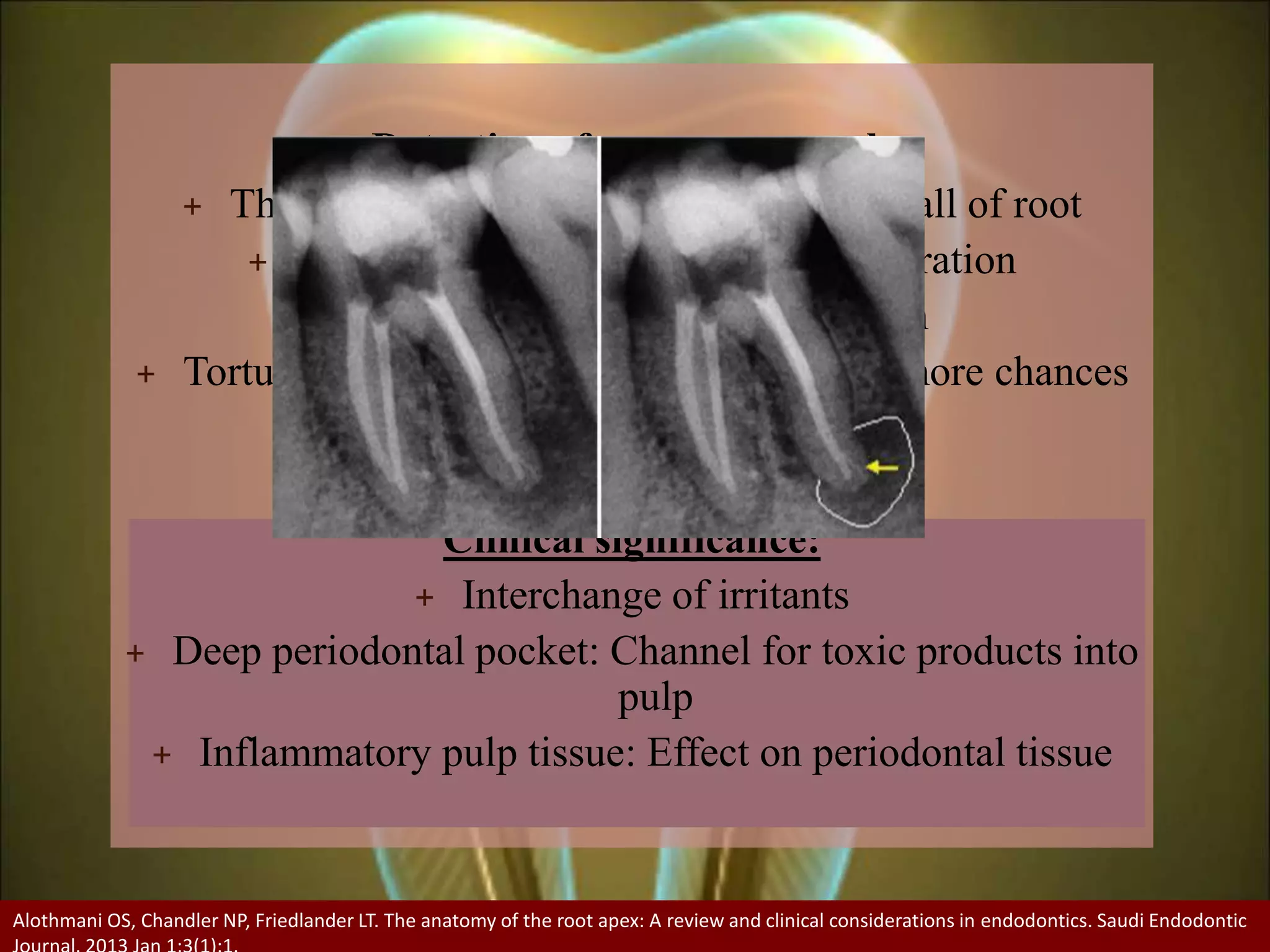
The document provides an extensive overview of dental pulp anatomy, including the history of pulp cavity research, classifications of root canals, and the significance of various anatomical features. It emphasizes the importance of understanding pulp variations for effective endodontic treatment and discusses the methodologies for studying pulp anatomy. Additionally, it highlights key anatomical laws governing pulpal morphology and includes classifications of both normal and pathological pulp anatomy.