The document provides a history of dental implants from ancient times to the modern era. Some key points discussed include:
- Ancient implants dating back to 400 BC made of materials like ivory and animal teeth.
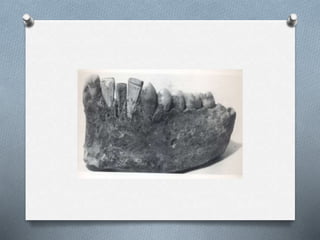
- Medieval period saw allotransplantation of animal teeth and use of materials like bone and ivory.
- Foundational period in the 1800s included early modern style root-form implants made of gold and other materials.
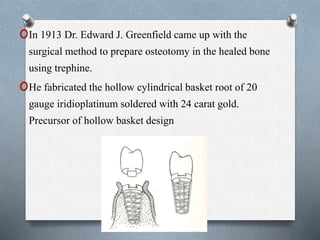
- Premodern era from 1910-1930 saw advances like Payne's silver capsule implant and Greenfield's hollow basket implant design.
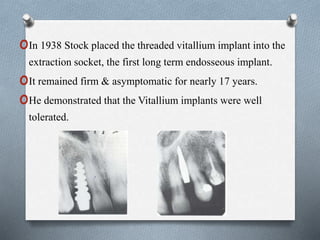
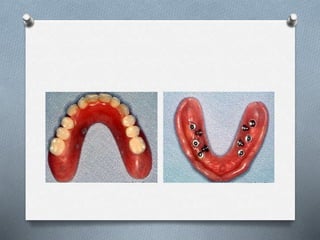
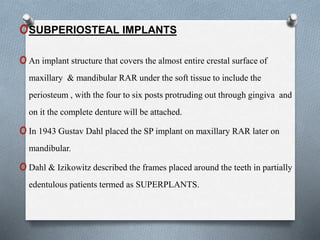
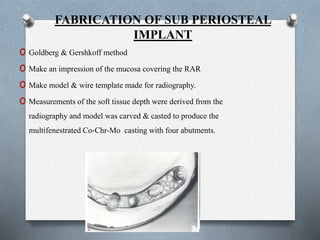
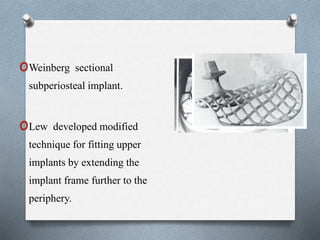
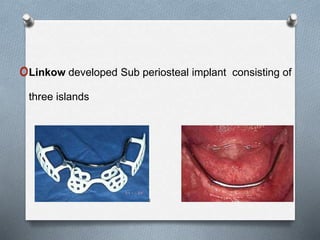
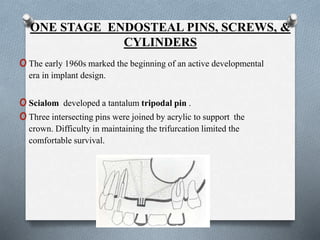
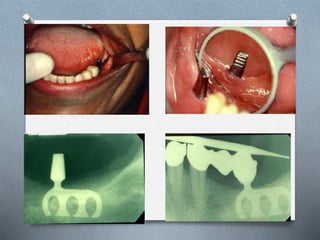
- Dawn of modern era from 1935 included developments like Strock's threaded vitallium implant and subperiosteal implant frames
































![Prosthodontic management of endodontically treated teeth [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/prosthodonticmanagementofendodonticallytreatedteethautosaved-210611115147-thumbnail.jpg?width=640&height=640&fit=bounds)
























































