Download to read offline


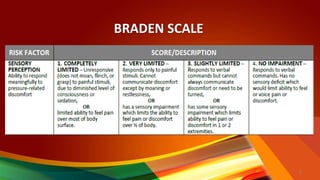
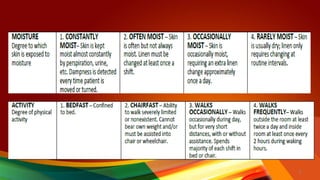
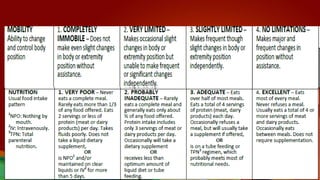


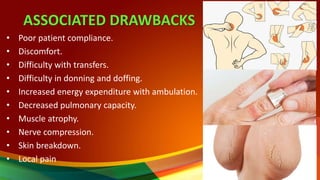
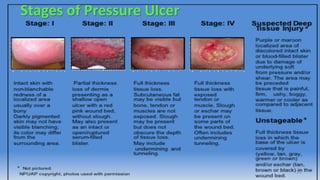
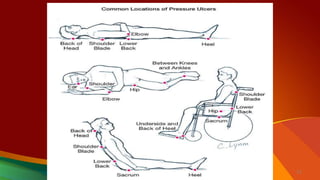

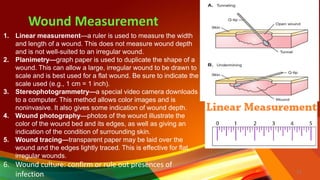


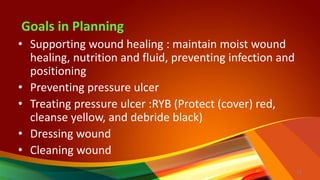
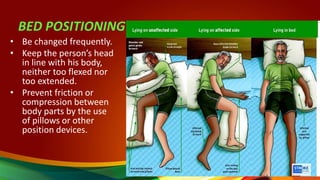


This document discusses integumentary integrity and wound assessment. It includes scales to assess risk of pressure sores, such as the Norton scale and Braden scale. Adaptive devices are designed for people with disabilities, while assistive devices can be used by anyone. Associated drawbacks of devices include skin breakdown. Wound assessment involves measuring the wound, reviewing skin characteristics, and checking for infection. Goals in wound care are supporting healing, preventing ulcers, and treating existing ulcers or wounds. Proper positioning and frequent repositioning are important to prevent skin issues.