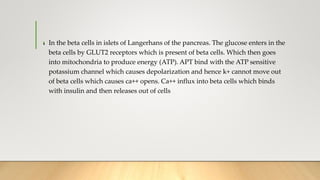
- Insulin is a hormone that allows glucose in the blood to enter cells, providing energy. It also helps break down fats and proteins for energy.
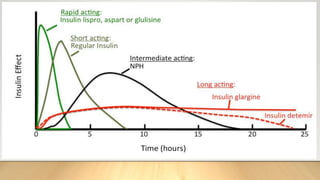
- There are different types of insulin that vary in how quickly they start working (onset), when they reach peak effectiveness, and how long their effects last. Fast-acting insulin works within 15 minutes, while long-acting insulin can work for up to 24 hours.
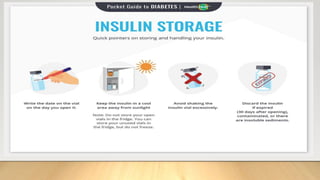
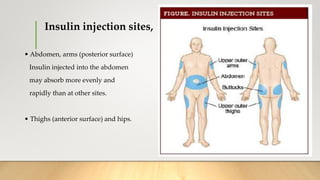
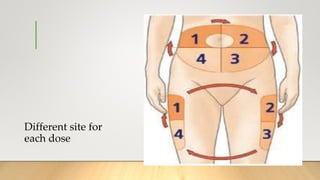
- Insulin is injected subcutaneously in areas like the abdomen, arms, thighs, and hips. Sites should be rotated and not used in the same spot for at least 2-3 weeks to prevent lumps. Proper storage and administration techniques are also important for safety and accuracy.
![.
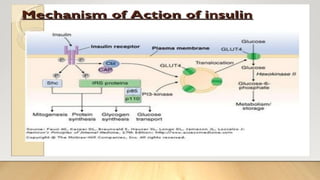
• Mechanism of action;
• Insulin binds with alpha subunit of insulin receptors on cell membrane. Beta
subunits of receptors become phosphorylate, phosphorylation of beta cells
activates local tyrosine kinase which then causes phosphorylation of multiple
other intracellular enzymes including insulin-receptor substrates [IRS]. IRS
stimulates Glucose transporter 4. glucose transporter acts as a channel and influx
of glucose from extracellular to intracellular.](https://image.slidesharecdn.com/insulin-191228174447/85/Insulin-by-Nurse-Practitioner-6-320.jpg)

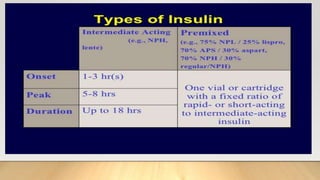
![INTERMIDIATE DURATION
THIS TYPE ENTERS THE BLOODSTREAM AT A SLOWER RATE BUT HAS A LONGER-LASTING
EFFECT. IT IS MOST EFFECTIVE AT MANAGING BLOOD SUGAR OVERNIGHT, AS WELL AS
BETWEEN MEALS.
OPTIONS FOR INTERMEDIATE-ACTING INSULIN INCLUDE:
NPH HUMAN INSULIN: [NEUTRAL PROTAMINE HEGEDORN ]
THIS TAKES BETWEEN 1 AND 2 HOURS TO ONSET, AND
REACHES ITS PEAK WITHIN 4 TO 6 HOURS. IT CAN LAST OVER 12 HOURS
IN SOME CASES. A VERY SMALL DOSE WILL BRING FORWARD THE PEAK
EFFECT, AND A HIGH DOSE WILL INCREASE
THE TIME NPH TAKES TO REACH ITS PEAK AND THE OVERALL DURATION
OF ITS EFFECT.](https://image.slidesharecdn.com/insulin-191228174447/85/Insulin-by-Nurse-Practitioner-14-320.jpg)