Indirect restorations are fabricated outside of the mouth using laboratory processed composites or ceramics. They are indicated for large defects or esthetic areas and provide better physical properties than direct composites. However, they have increased costs and time. Tooth preparation for indirect restorations requires rounded line angles, occlusal convergence, and extension to sound tooth structure. Impressions are needed to fabricate the restoration on a working cast.



![INDICATIONS
◦ The indications for Class I and II indirect tooth-colored restorations are
◦
◦ 1]Esthetics-Indicated for Class I and II restorations located in areas of esthetic
importance for the patient.
◦ 2] Large defects or previous restorations—They are considered for
restoration of large Class I and II defects or replacement of large
compromised existing restorations, especially those that are wide facio-
lingually and require cusp coverage.
Sturdevant’s ED 5](https://image.slidesharecdn.com/indirectrestorations-230917150013-163e18cc/85/INDIRECT-RESTORATIONS-pptx-4-320.jpg)
![INDICATIONS
◦ Indirect tooth-colored restorative materials are more durable than direct
composites when placed in large occlusal posterior restorations, especially in
regard to maintaining occlusal surfaces and occlusal contacts.[Söderholm etal]
◦ The wear resistance provided by indirect materials is especially important in
large posterior restorations that involve most or all of the occlusal contacts
[Sturdevant etal]
◦ Economic factors—Some patients desire the most esthetic dental treatment
available, regardless of cost
Sturdevant’s ED 5](https://image.slidesharecdn.com/indirectrestorations-230917150013-163e18cc/85/INDIRECT-RESTORATIONS-pptx-5-320.jpg)

![Contraindications
◦ 1] Heavy occlusal forces—Ceramic restorations can fracture when they lack
sufficient bulk or are subject to excessive occlusal stress, as in patients who
have bruxing or clenching habits
◦ 2] Inability to maintain a dry field.
◦ 3] Deep subgingival preparation.
◦ These margins are difficult to record with an impression and are difficult
to finish.
Sturdevant’s ED 5](https://image.slidesharecdn.com/indirectrestorations-230917150013-163e18cc/85/INDIRECT-RESTORATIONS-pptx-7-320.jpg)








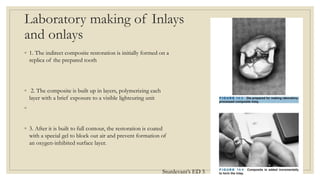
![Laboratory-Processed Composite Inlays and
Onlays
Processed composite restorations are indicated when
1] Maximum wear resistance is desired from a composite restoration,
2]Achievement of proper contours and contacts would be difficult otherwise,
3] The indirect composite likely would cause less wear of the opposing dentition than a similar ceramic
restoration
Sturdevant’s ED 5](https://image.slidesharecdn.com/indirectrestorations-230917150013-163e18cc/85/INDIRECT-RESTORATIONS-pptx-16-320.jpg)



















































![Cast gold CERAMIC composite
Cast gold usually made of 10 to 22
carats gold , copper, silver ,
palladium, platinum, nickel, zinc.
INDICATIONS
1. Extensive tooth loss, Correction of
occlusion
2. Restoration of endodontically treated
teeth
3. Preexisting cast metal restorations
CONTRAINDICATIONS
1. Occlusal disharmony
2. Dissimilar metals
Ceramic restorations, also known
as porcelain restorations, are made
of dental-grade ceramic materials.
1.ESTHETICS
2.PRESERVATION OF TOOTH
STRUCTURE
1]Heavy occlusal forces
2] Inability to maintain a dry field.
3] Deep subgingival preparation.
Resin composite restorations are
made of a mixture of plastic
(composite resin) and fine glass
particles
1. .ESTHETICS
2.WORN OUT TOOTH
3]BRUXISM
4]ALLERGY](https://image.slidesharecdn.com/indirectrestorations-230917150013-163e18cc/85/INDIRECT-RESTORATIONS-pptx-76-320.jpg)
![Cast gold CERAMIC composite
ADVANTAGES
1.Greater tensile strength
2.Precise reproduction of the form and
minute details
3.Metal alloys used are tarnish and
corrosion resistant
4. Finishing and polishing can be done
outside the oral cavity, thus preventing
damage to the pulp
DISADVANTAGES
1. Leakage around and under the
restorations through the cement-
restoration - tooth junction
2.It involves extensive tooth preparation
3.Technique sensitive
4. Galvanic deterioration
1]Wear resistance—Ceramic restorations
are more wear resistant than direct
composite restorations.
Ability to strengthen remaining tooth
structure
3]More precise control of contours and
contacts
4]Biocompatibility and good tissue
response
1]Brittleness of ceramics.
2]Wear of opposing dentition and
restorations
3]Resin-to-resin bonding difficulties
4]Low potential for repair
1]Bonding and reinforcement
2]Reduced sensitivity
3]Repairability
4]Conservative tooth preparation
5]Biocompatibility
1]Durability
2]Staining and discolouration
3]less lifespan
4]technique sensitive
5]limited strength in large restorations](https://image.slidesharecdn.com/indirectrestorations-230917150013-163e18cc/85/INDIRECT-RESTORATIONS-pptx-77-320.jpg)
![Cast gold usually made of
copper, silver, platinum, nickel,
zinc
Gold offers high strength and
durability.
They are more suitable for
posterior teeth where esthetics
are not a primary concern
Ceramic restorations, also
known as porcelain restorations,
are made of dental-grade
ceramic materials.
They are generally not as strong
as metal restorations.
They are highly esthetic and are
commonly used in the front
teeth.
Resin composite restorations
are made of a mixture of plastic
(composite resin) and fine glass
particles
They are generally not as strong
as ceramics or metals.
They offer excellent esthetics
and are commonly used in both
front and back teeth.
Cast gold CERAMIC composite
LUTING CEMENT:
Zinc phosphate cement provides good
retention and is particularly useful for
cast gold restorations due to its ability
to bond to both metal and tooth
structure[Donovan and Cho, 1999]
TOOTH PREPERATION:
Bevel is needed
Cast gold inlays, a slight divergence or
taper of 2 to 5 degrees is required
Occlusal Reduction:1.5-2 mm
Resin cements are widely used for
luting ceramic restorations due to their
excellent adhesive properties and
esthetics
Bevel is usually not recommended
The divergence angle of more than[ 2 to
5]. helps ensure a secure fit and stability
of the restoration within the tooth
preparation
1.5 to 2mm.
Resin cements used for composite inlays
are typically dual-cured or light-cured
[el-Mowafy et al. ]
Bevel not needed.
The divergence angle of [more than 2 to
5 degrees] same as ceramic
1.5 to 2mm](https://image.slidesharecdn.com/indirectrestorations-230917150013-163e18cc/85/INDIRECT-RESTORATIONS-pptx-78-320.jpg)

![Cast gold CERAMIC composite
Biocompatibility is good
ADAPTABILITY
Gold restorations are more
adaptable
LONGEVITY
Gold restorations known for their
durability [Leempoel et al. ]
TYPE OF TOOTH PREP
Gold restorations usually require
less tooth removal
Dental ceramics are generally
biocompatible
Ceramics are difficult to adapt
Ceramic restorations are known
for their excellent long-term
durability[Wendt SL etal]
Ceramic restorations may require
more tooth structure removal
They are also biocompatible
Composites are also difficult to
adapt
They tend to have a shorter
lifespan compared to ceramic
restorations. [Taylor DF, et al]
Resin composite restorations
require less tooth structure
removal](https://image.slidesharecdn.com/indirectrestorations-230917150013-163e18cc/85/INDIRECT-RESTORATIONS-pptx-80-320.jpg)