





























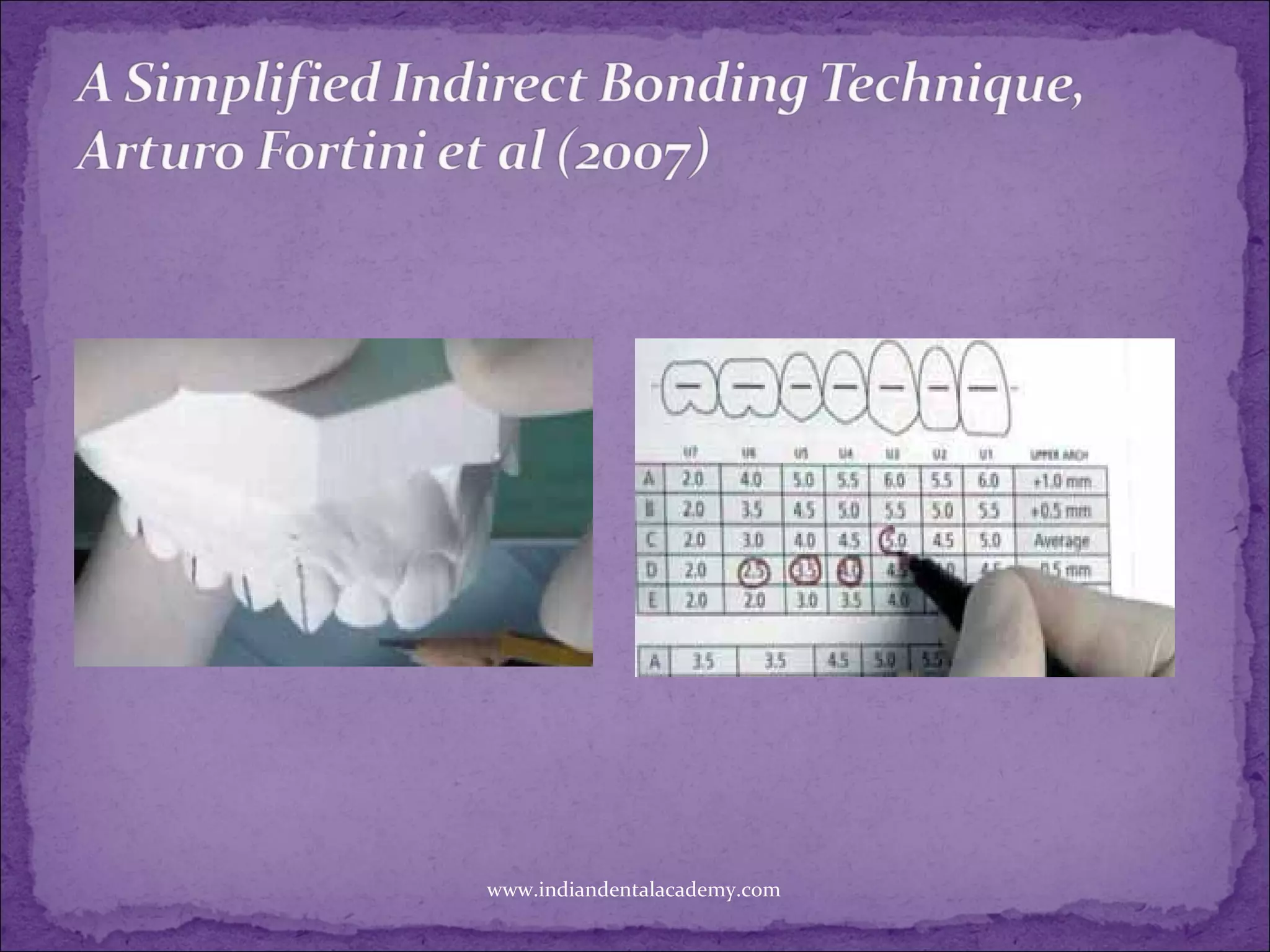

















The document discusses the technique of indirect bonding in orthodontics, detailing its history and evolution since it was first described in 1972. It covers various methods and materials used, the advantages of indirect bonding such as reduced chair time and improved aesthetics, as well as challenges it faces, such as bonding limitations on certain tooth types. Additionally, it compares the effectiveness of direct versus indirect bonding methods in terms of bond strength and accuracy of bracket placement.