This document discusses enamel preparation and self-etching primers for orthodontic bonding. It begins with an introduction to bonding materials and techniques. It then discusses cleaning and conditioning the enamel surface, including using self-etching primers that combine conditioning and priming into a single step. Lastly, it covers the bonding procedure and types of adhesives, brackets, and ligation methods used for orthodontic bonding.




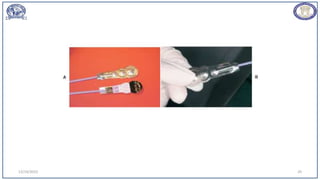




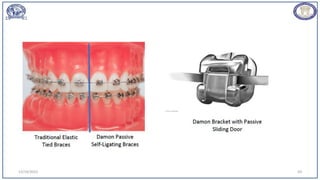
![• Several types of ligature-less, self-ligating, low-friction brackets have become
available in recent years (e.g.,SPEED System [Strite Industries, Cambridge, Ontario],
Damon Q [Ormco], Smartclip SL3 [3M/Unitek]).
• The popularity of these brackets seems to be increasing.1 Such brackets may offer
the advantages of saving time, reducing friction, and
probably increasing patient comfort.
12/19/2023 58](https://image.slidesharecdn.com/enamelpreparationandselfetchingprimer-231219154201-da890808/85/enamel-preparation-and-self-etching-primer-pptx-58-320.jpg)


























































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)











