Downloaded 349 times
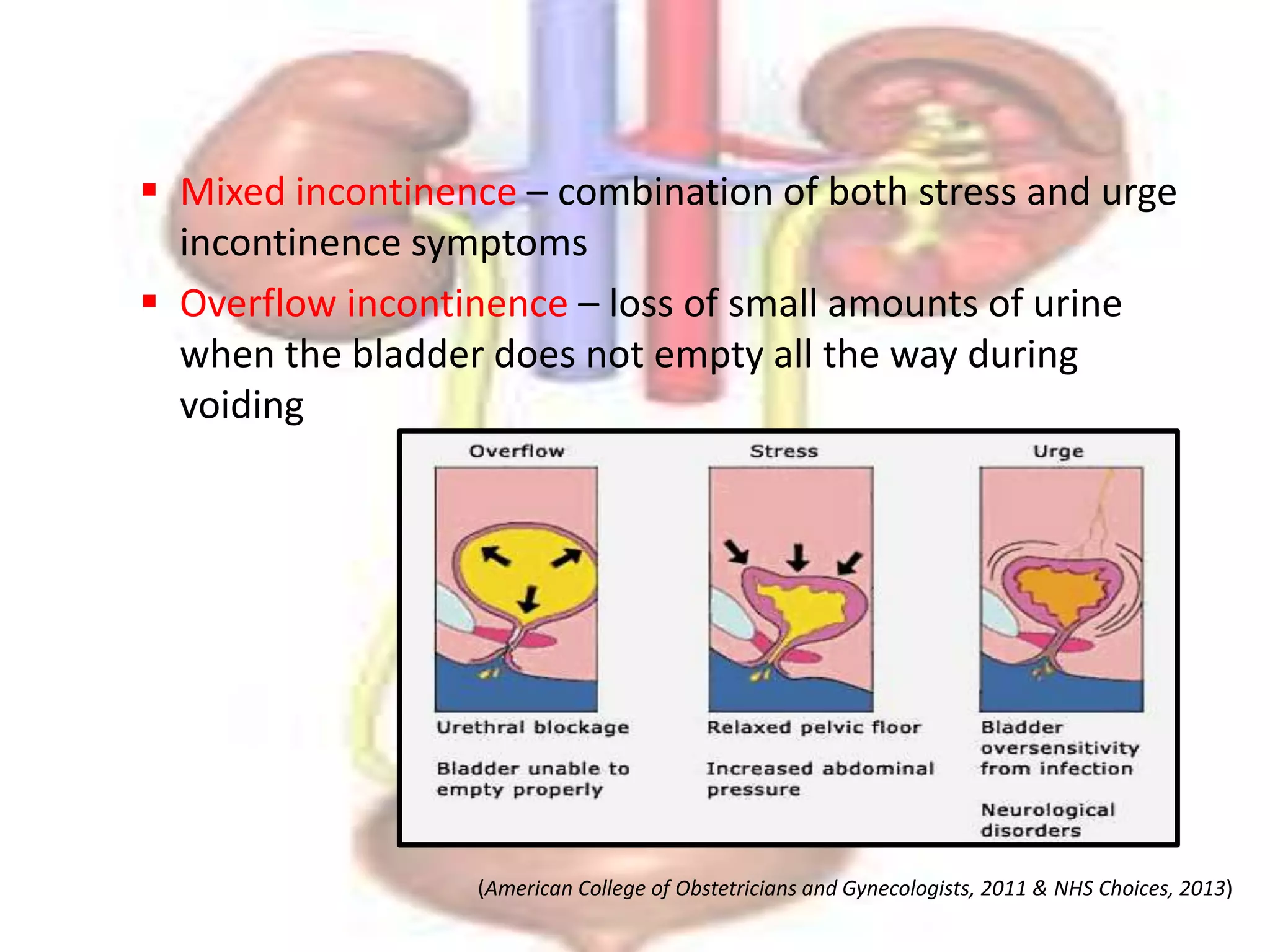

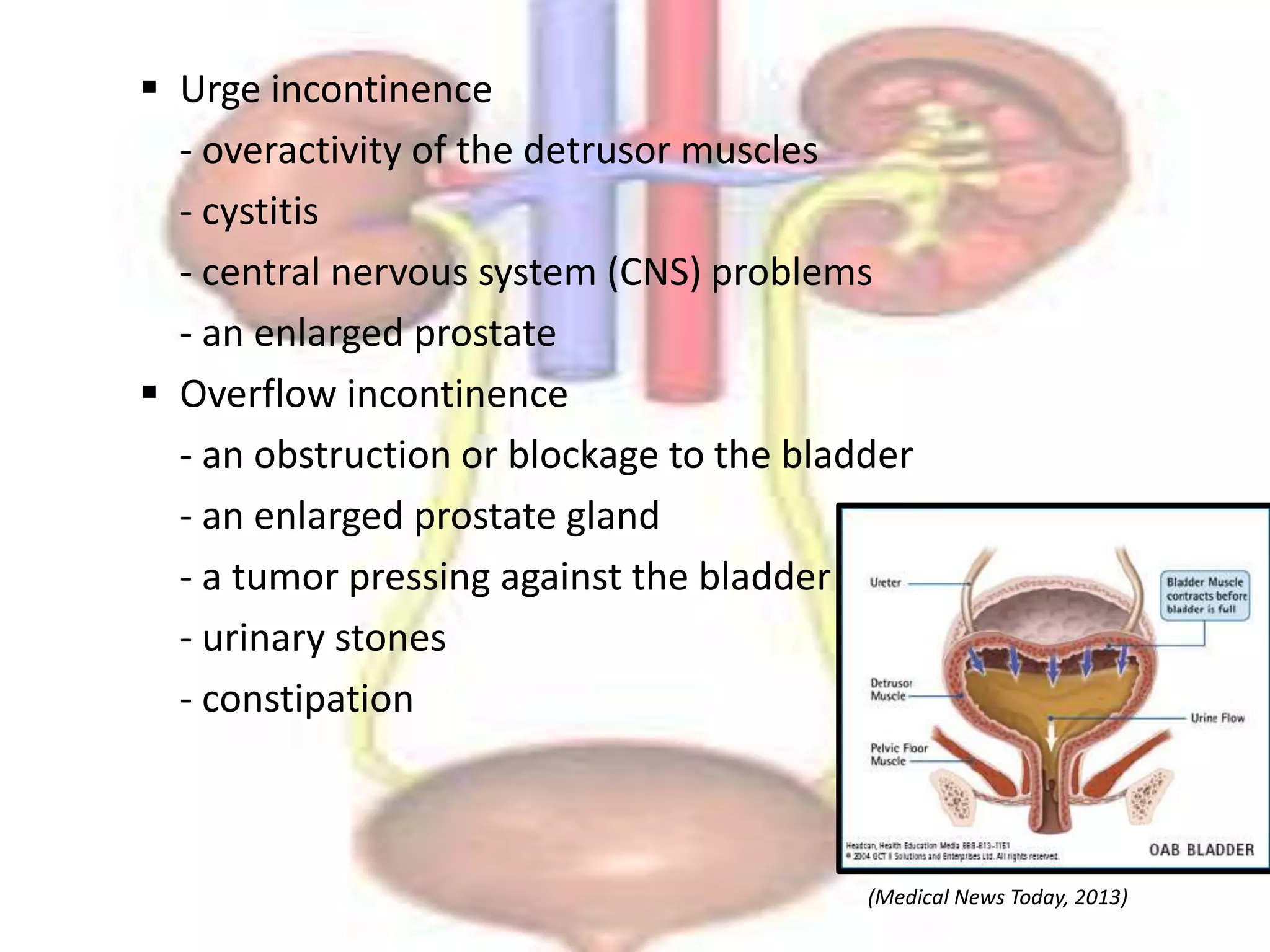
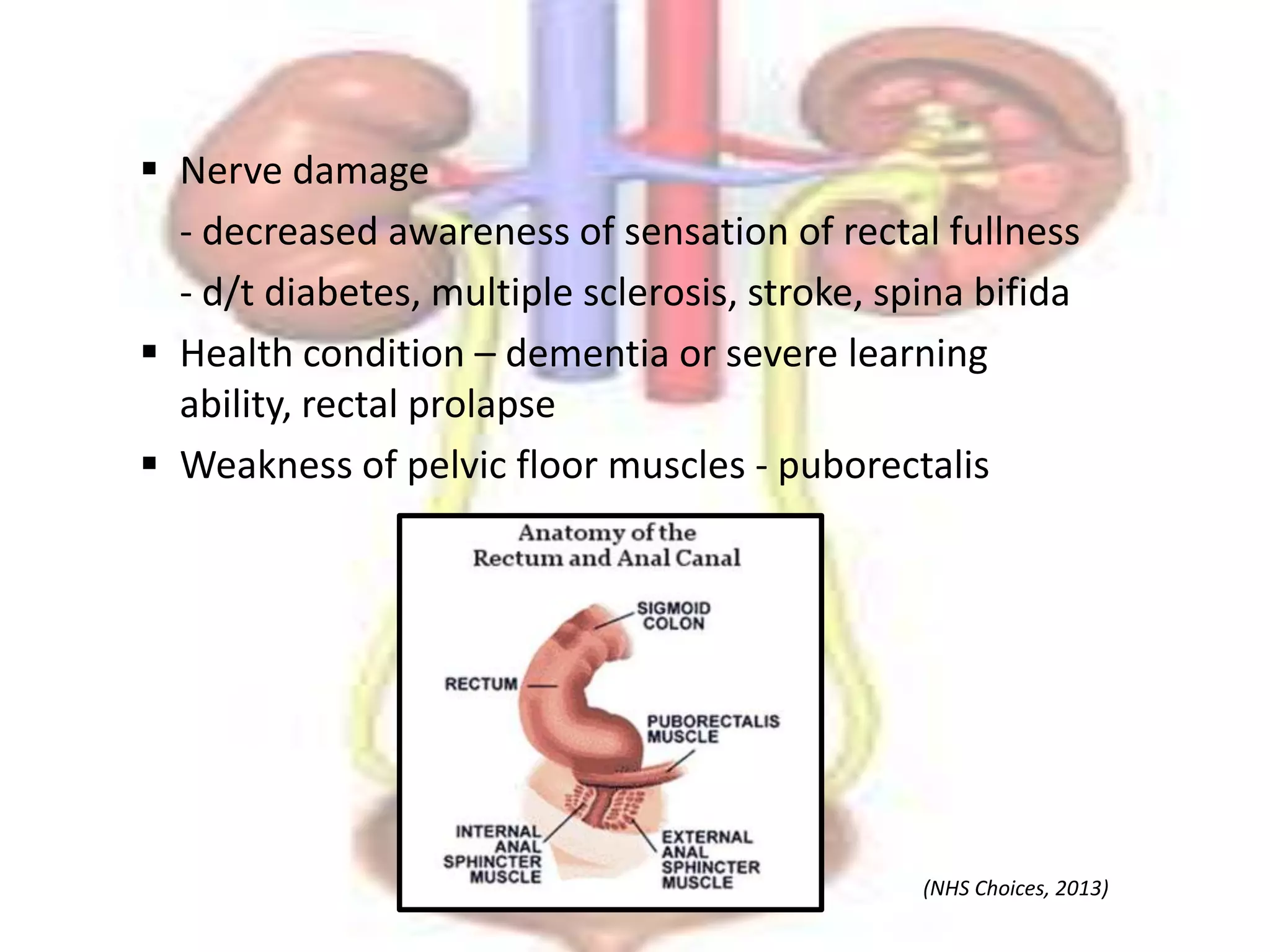









This document discusses bladder and bowel incontinence. It defines the different types of each condition and describes their causes, clinical features, and management. Bladder incontinence types include stress, urge, mixed and overflow incontinence. Causes involve weakening of pelvic floor muscles from childbirth, surgery, or age. Bowel incontinence results from issues with the rectum, sphincter muscles, or nerves. Clinical features and management by medications, devices, surgery, and physiotherapy exercises are outlined.























































































