Downloaded 30 times





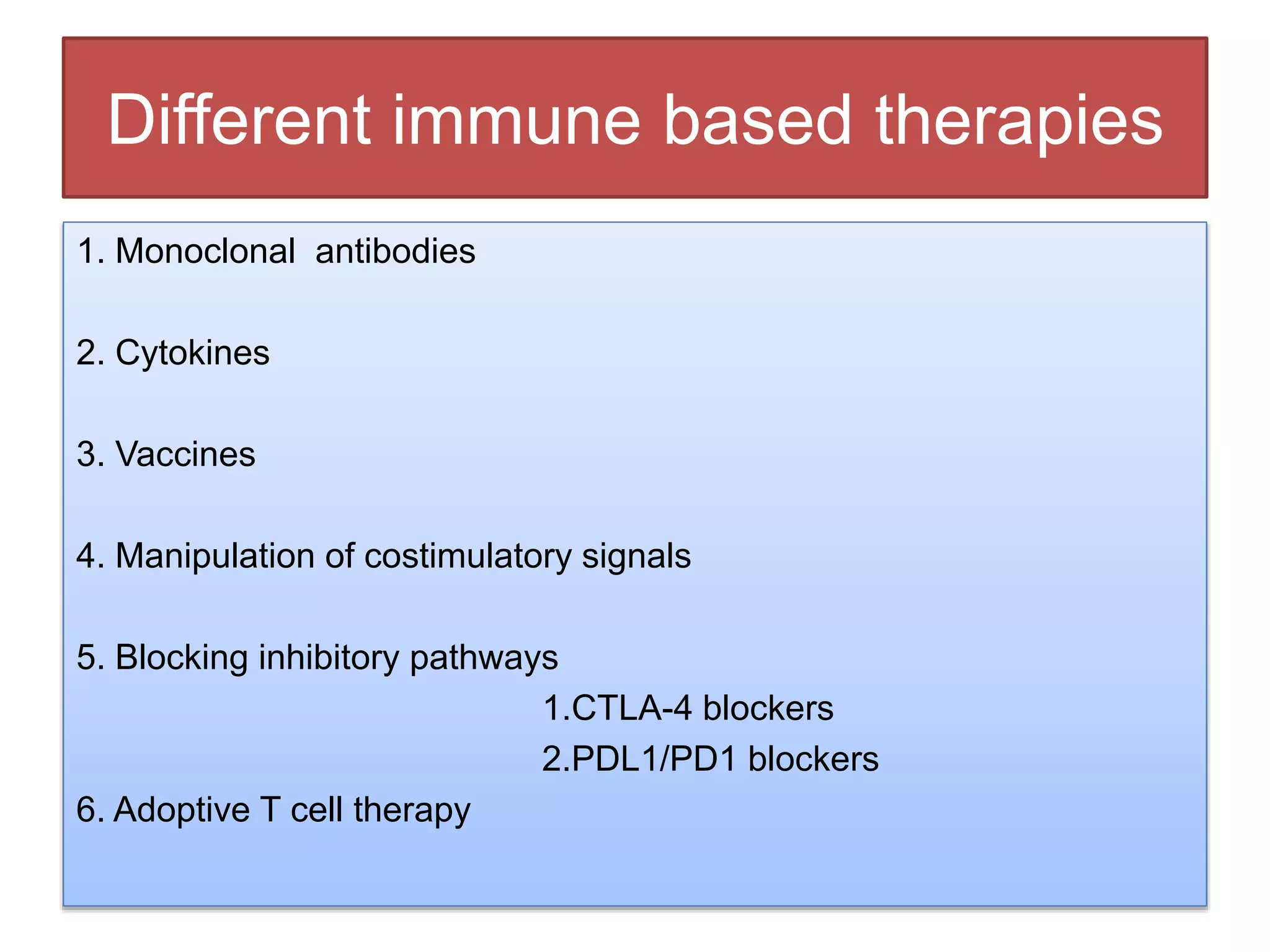


























This document discusses adaptive immunity in cancer therapies. It provides an overview of the history of cancer immunotherapy from ancient times to modern immunotherapy approaches. It describes the key players in the anti-tumor immune response including T cells, B cells, macrophages, and dendritic cells. Different immune-based therapy approaches are summarized, including monoclonal antibodies, cytokines, vaccines, manipulation of costimulatory signals, blocking inhibitory pathways, adoptive T cell therapy, and oncolytic virotherapy. The conclusion states that immunotherapy has shown effectiveness for some cancer types but has not been proven as an effective sole treatment for cancer.