Downloaded 96 times



























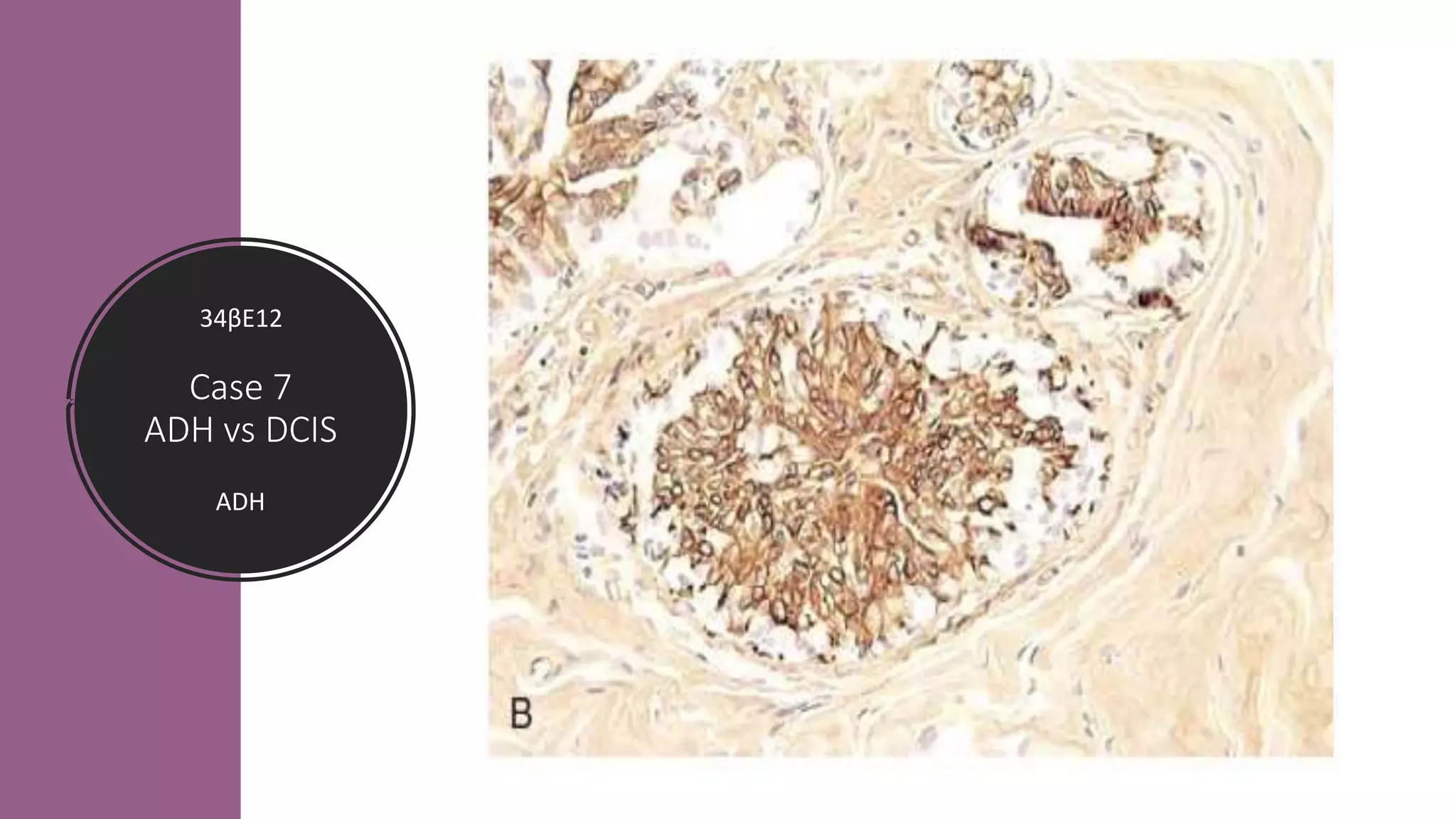





































1. The combination of SMMHC and p63 is ideal for marking myoepithelial cells and assessing features such as stromal invasion and differentiation of in situ versus invasive lesions. 2. Positive 34βE12 and CK5/6 staining within the proliferative component indicates atypical papilloma rather than papilloma with DCIS. 3. Intracystic papillary carcinoma shows positive staining by Collagen IV around ducts, distinguishing it from solid papillary carcinoma.























































































