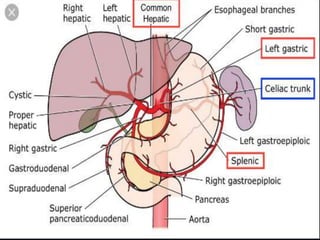
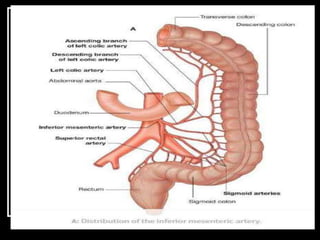
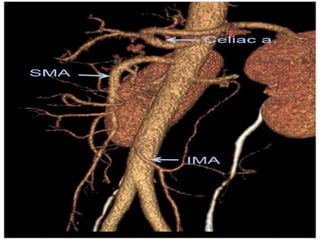
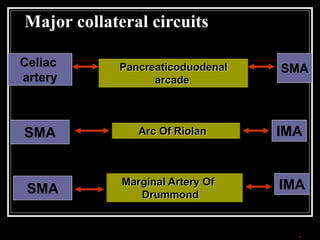
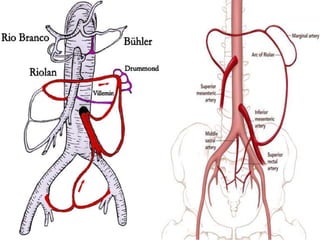
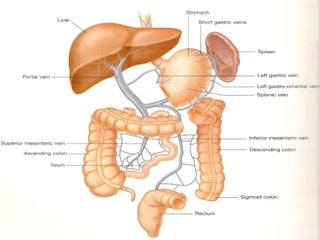
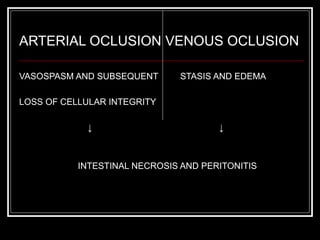
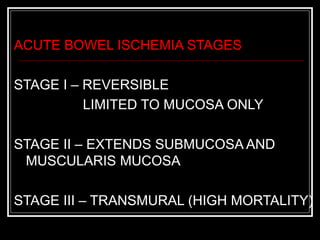
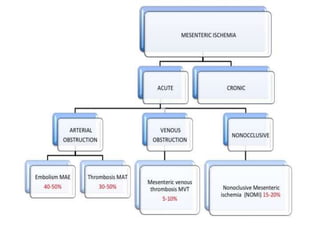
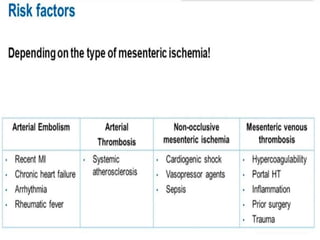
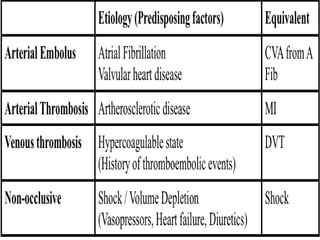
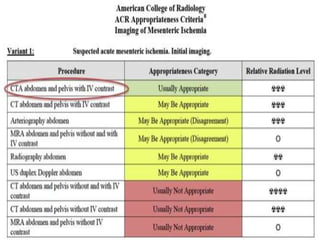
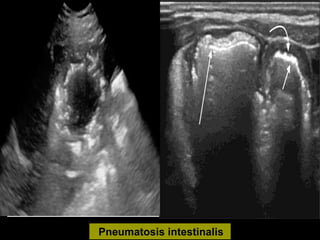
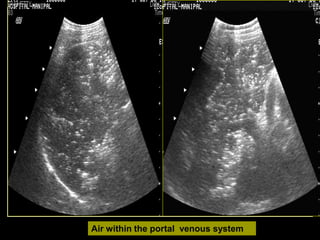
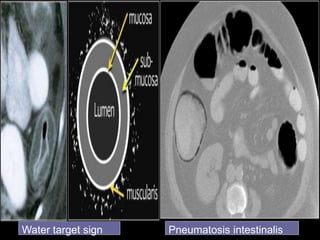
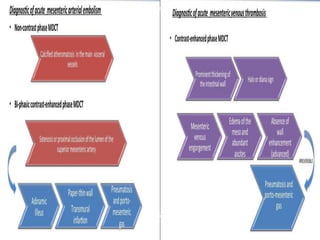
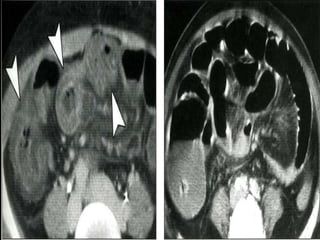
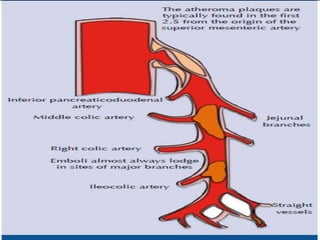
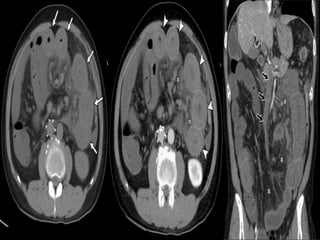
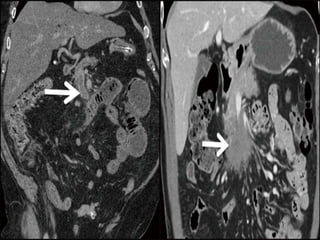
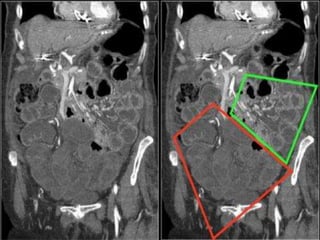
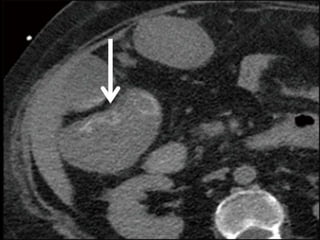
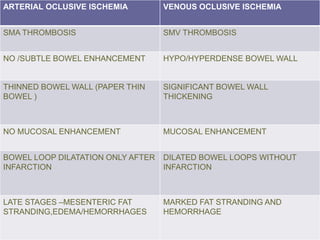
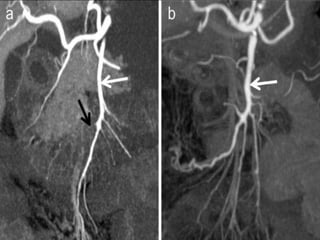
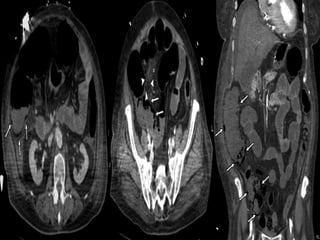
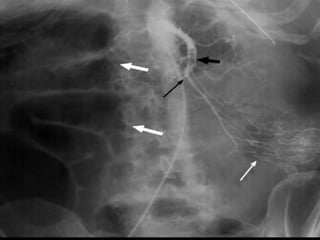
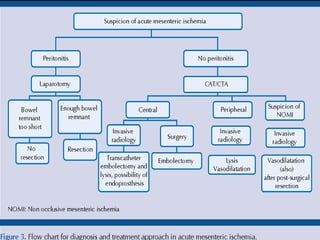
This document discusses imaging in bowel ischemia. It provides an overview of the anatomy of the splanchnic circulation and mesenteric arteries/veins. It then covers the pathophysiology, causes, clinical features, and imaging findings of both acute and chronic mesenteric ischemia. For imaging, it discusses the role of plain radiography, ultrasound and Doppler, CT, angiography, and MRI. It provides examples of imaging findings for different types of mesenteric ischemia and highlights how each modality can help in diagnosis.