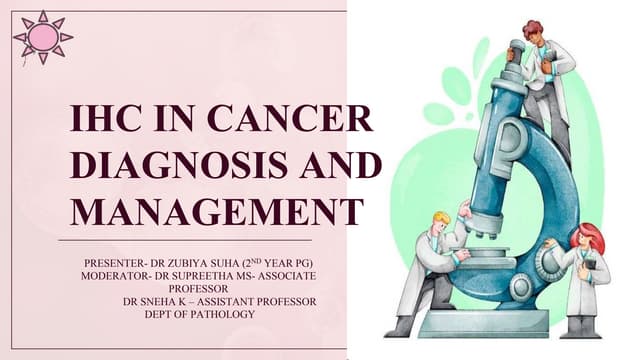
![Purpose of IHC
Purpose 目的 Example
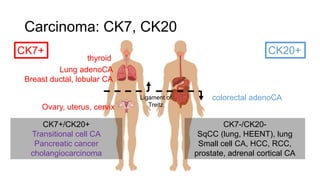
Classification of tumors
區分腫瘤
carcinoma vs. lymphoma
B cell vs. T cell lymphoma
in situ lesions vs. invasive carcinomas
原位癌 或 侵襲癌
myoepithelial markers in breast cancers
basal cell markers in prostate
Prognostic factors
預後因子
Ki-67 in glioblastomas (GBM)
Predictive factors for specific therapy
標靶治療效果預測
c-KIT
ER, PR, HER2/neu
Identification of extracellular material
胞外物質
β-2 microglobulin amyloid
Identification of infectious agents
傳染性物質
CMV or HSV
[整理自: Susan Lester, Manual of Surgical Pathology 3e]](https://image.slidesharecdn.com/ihc-171106053130/85/IHC-4-320.jpg)
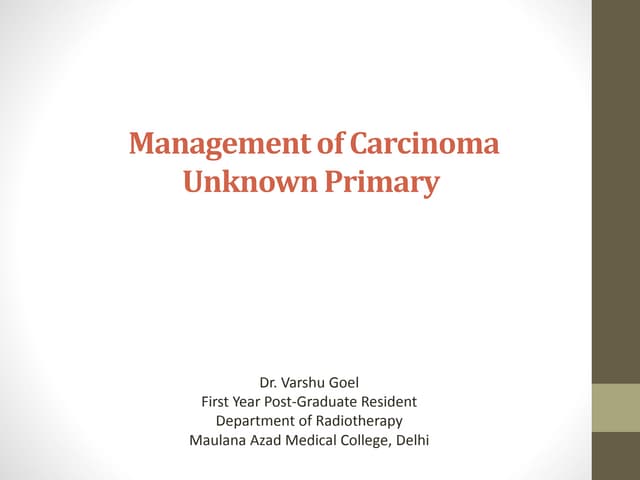
![IHC applications -1
Application Tumor markers
Histological typing Carcinoma Cytokeratin
Sarcoma Vimentin
Glial tumor GFAP
Melanoma HMB-45,
Melan-A
Lymphoma LCA
Differentiation
Sarcoma
Liposarcoma S-100
Angiosarcoma CD31
factor VIII
Leiomyo-
sarcoma
SMA
Rhabdomyo-
sarcoma
Desmin
[Note from Ming-Yuan Lee, M.D.’s Lecture]
Application Tumor/site Markers
Organ specific Thyroid Thyroglobulin
prostate PSA
Lung, thyroid TTF-1
Sub-
classification
B-cell CD20, CD79a
T-cell CD3, CD5, CD43
NK cell CD56
Myeloid
series
MPO
Infectious
disease
- CMV
Lung PJP](https://image.slidesharecdn.com/ihc-171106053130/85/IHC-5-320.jpg)
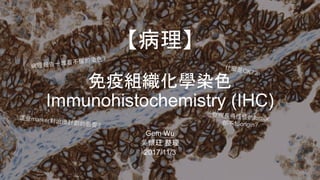
![IHC applications -2
Application Tumor markers
Secretion or
tumor
products
Adenocarcinoma CEA
Neuroendocrine tumor Synaptophysin,
insulin, gastrin
Breast tumor BRST-2
HCC α-fetoprotein,
Hepar-1
Choriocarcinoma β-HCG
Yolk sac tumor or
embryonal carcinoma
α-fetoprotein
Biological
factors for
prognostic
values
(Proliferation index) Ki-67
(anti-apoptotic factor) Bcl-2
(Poor prognosis) Her2
[Note from Ming-Yuan Lee, M.D.’s Lecture]
Application Treatment marker
s
Therapy Tamoxifen ER/PR
Herceptin HER2
Gleevec CD117
Erlotinib
(Tarceva®)
EGFR
Pem-
brolizumab
PD-L1
不同的organ, standard不同
Lymphoma 50% Ki-67+可能只是moderate,
但breast可能就是high](https://image.slidesharecdn.com/ihc-171106053130/85/IHC-6-320.jpg)
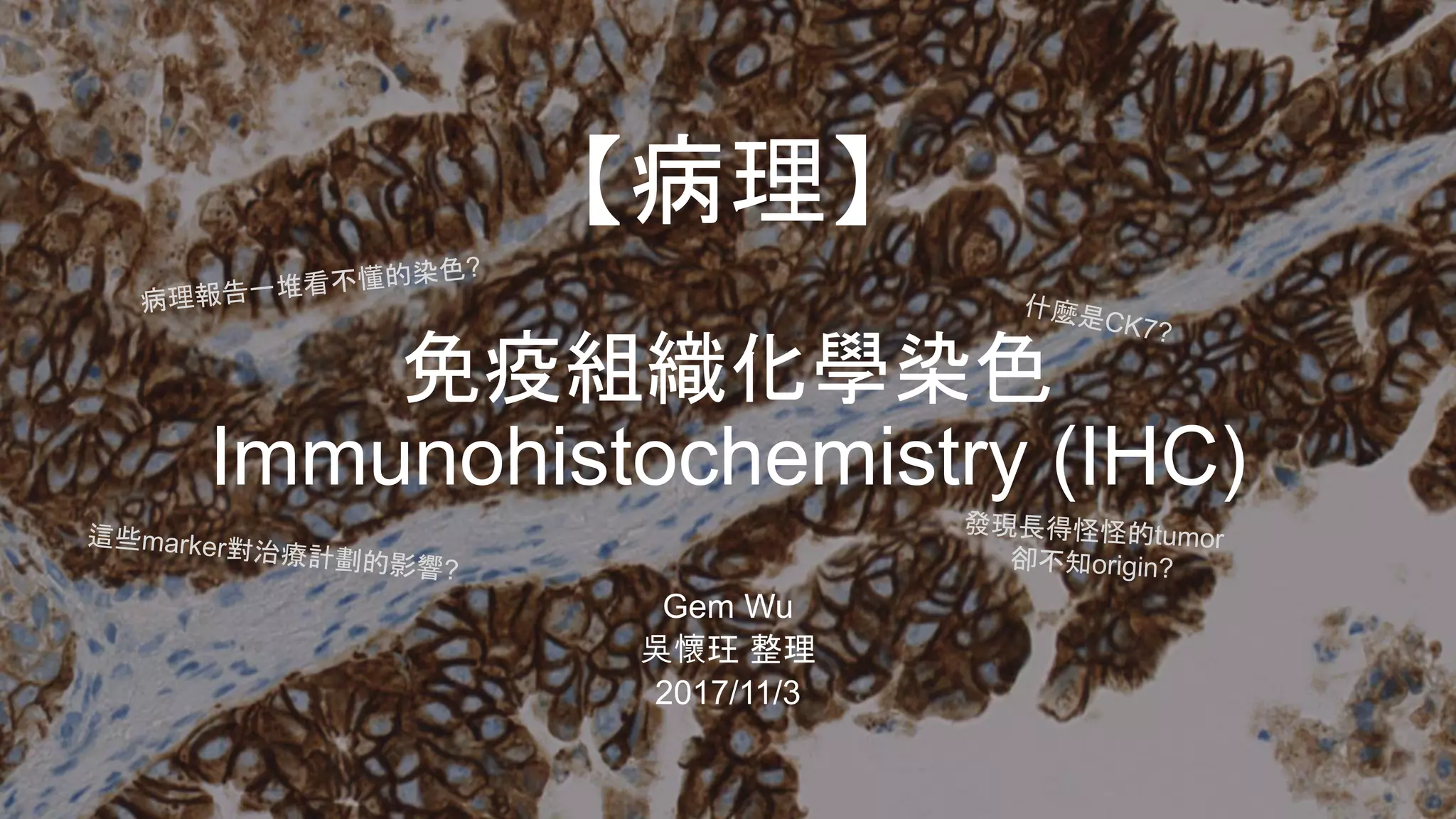
![Organ specific markers of carcinoma
Breast Cancer – IHC有助規劃Treatment
IHC result ER/PR HER2/neu
Positive 70-80% 15-20%
Borderline 5-10% 25-35%
Negative 20-30% 70%
[來自: Susan Lester, Manual of Surgical Pathology 3e]
HER2/neu+ → 可用Herceptin治療
↓ HER2/neu+用IHC(左)與ISH(右)
Other markers: (如果不確定可以三個一起染)
GCDFP-15, mammaglobin, GATA3…
[Arch Pathol Lab Med. 2016;140:508–523; doi: 10.5858/arpa.2015-0173-CP)]](https://image.slidesharecdn.com/ihc-171106053130/85/IHC-9-320.jpg)
![Organ specific markers of carcinoma
Lung Cancer – IHC分辨不同類型
tumor CK7 CK20 TTF-1 P63 Chromogranin
Adenocarcinoma 90+% 10-40% 60-90% 10-40% <10%
Bronchioloalveolar
carcinoma — nonmucinous
90+% 10-40% 60-90% 60-90% <10%
Bronchioloalveolar
carcinoma — mucinous
60-90% 60-90% 10-40% <10%
Squamous cell carcinoma 10-40% <10% <10% 90+% <10%
Large cell carcinoma 60-90% 10-40% 40-60% 40-60% <10%
Small cell carcinoma 10-40% <10% 90+% <10% 40-60%
Carcinoid tumor 40-60% <10% 10-40% <10% 90+%
Metastatic colon carcinoma 90+% 10-40% <10% <10% <10%
Metastatic breast carcinoma 90+% <10% <10% <10% <10%
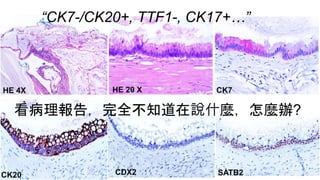
通常會染TTF-1來確認lung origin,但總有些例外…
[整理自: Susan Lester, Manual of Surgical Pathology 3e]
Neuroendocrine
tumor marker](https://image.slidesharecdn.com/ihc-171106053130/85/IHC-10-320.jpg)
![Organ specific markers of carcinoma
GI tract Cancer v. GYN cancer – 確認origin
CDX2 is expressed in virtually 100% of colorectal adenocarcinomas.
(除了MSI – microsatellite unstable genotype外)
tumor CK7 CK20 MUC2 CDX2 WT-1
Stomach 60-90% 40-60% 40-60% 40-60% 40-60%
pancreas 90+% 60-90% 90+% 40-60% 40-60%
appendix 10-40% 90+% 90+% 90+% -
Colon <10% 90+% 60-90% 90+% 60-90%
Uterus 90+% 10-40% <10% 10-40% 40-60%
Ovary, serous 90+% 10-40% 10-40% 40-60% 60-90%
Ovary, mucinous 90+% 60-90% 10-40% 40-60% 10-40%
Breast, no special type (NST) 90+% <10% 10-40% <10% 10-40%
Breast, mucinous 90+% 10-40% 90+% - 60-90%
[整理自: Susan Lester, Manual of Surgical Pathology 3e]
1
2
3
4
5
6
PAX-8是Müllerian duct轉錄因子,因此許多GYN tumor會表現,也可以此區別mets的breast CA v. primary](https://image.slidesharecdn.com/ihc-171106053130/85/IHC-11-320.jpg)
![Organ specific markers of carcinoma
Liver Cancer – 區分primary或metastasis
Hep-Par 1 Ab, arginase-1 比傳統的 α-FP更sensitive與specific for HCC
[圖來自: Susan Lester, Manual of Surgical Pathology 3e]
Hepatoplastoma Cholangiocarcinoma
? ?CK7+, AE1/AE3+,
keratin HMW+
一般來說,liver primary cancer會有CAM5.2+, CK20-, CEA+
CD10+
cirrhosis (65-90%)
↓ HBV+ (50%)
α-FP+, HEP+
CDX2+
HEP+
[Arch Pathol Lab Med. 2016;140:508–523; doi: 10.5858/arpa.2015-0173-CP)]](https://image.slidesharecdn.com/ihc-171106053130/85/IHC-12-320.jpg)
![Other markers for carcinomas
Prostate CA
(NKX3.1)
(PSA)
TCC
(GATA3)
(Uroplakin)
(p63, p40)
RCC
(PAX2)
(PAX8)
Thyroid papillary,
follicular CA
(Thyroglobulin)
(PAX8)
Most thyroid CA
(TTF-1)
adrenal CA
(inhibin-α)
(Melan-A)
(Steroidogenic
factor 1)
SqCC (not organ specific)
(p63+, p40+)
(CK5)[Arch Pathol Lab Med. 2016;140:508–523; doi: 10.5858/arpa.2015-0173-CP)]](https://image.slidesharecdn.com/ihc-171106053130/85/IHC-13-320.jpg)
![Case 1
• Ex-smoker
• Biopsy from
left lower
lobe of lung
• w/ Hx of
biopsy
proven colon
CA
• Dx?
CK20+++H&E
CDX2+++ TTF1-
(CK7-)
[Arch Pathol Lab Med. 2016;140:508–523;
doi: 10.5858/arpa.2015-0173-CP)]](https://image.slidesharecdn.com/ihc-171106053130/85/IHC-15-320.jpg)
![[CASE2]
63M, no known primary carcinoma, CCx cervical
lymphadenopathy, this is the result of FNA of the node:
CK7-, CK20-, TTF1-, CDX2-, PSA+++, Villin-. Dx?
[CASE3]
73F, hx hysterectomy for unknown reason, CCx retroperitoneal
lymphadenopathy, image showed left pelvic sidewall mass probably
residual ovary. this is the FNA result:
ER++, WT++, PAX+++, CK7+++, CK20-, GATA3-, CDX2-, p63-. Dx?
[Arch Pathol Lab Med. 2016;140:508–523; doi: 10.5858/arpa.2015-0173-CP)]](https://image.slidesharecdn.com/ihc-171106053130/85/IHC-16-320.jpg)

This document discusses immunohistochemistry (IHC), which helps pathologists further characterize and classify tumors seen on histopathology slides. It provides examples of how IHC is used to distinguish between different tumor types like carcinoma vs lymphoma, classify tumors by origin like breast vs gastrointestinal cancers, and provide prognostic or predictive information about tumor biology and targeted therapies. Specific IHC markers are discussed that are useful for different tumor sites like lung, breast, prostate, liver and gastrointestinal cancers. The limitations of IHC are also noted, as positive and negative results still require correlation with other histologic and clinical findings.