Downloaded 921 times
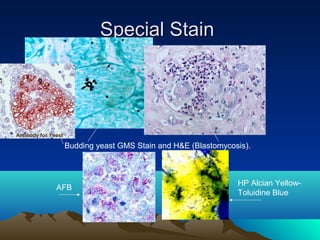
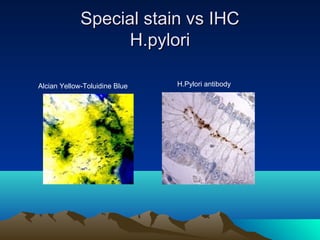
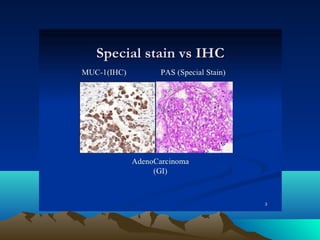
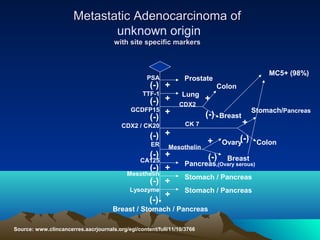
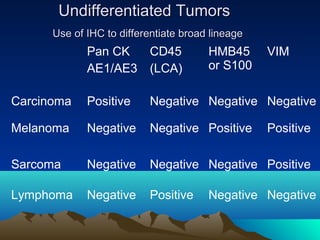
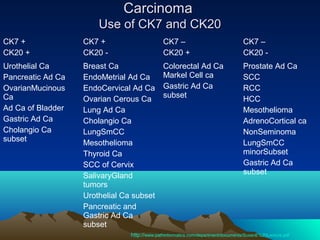
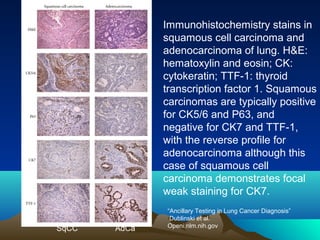
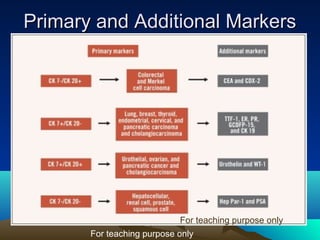
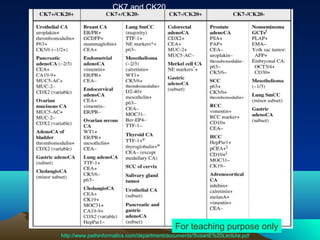
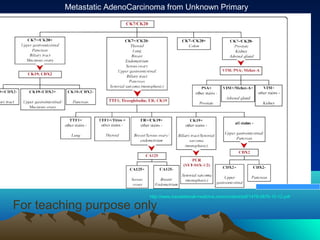
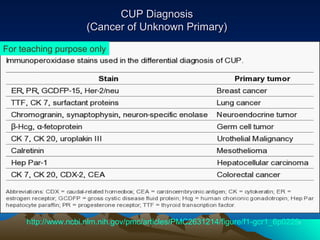
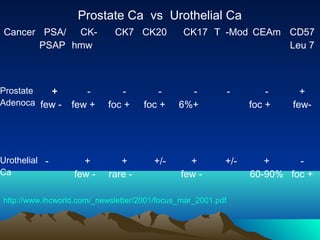
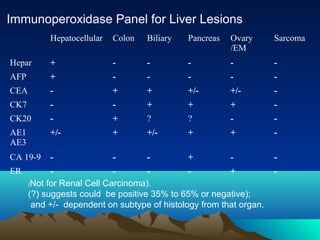
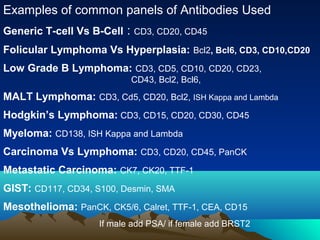
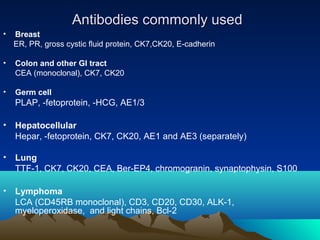
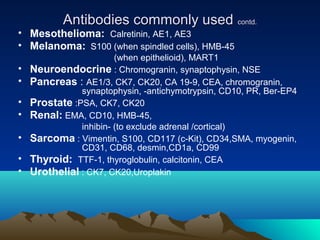


IHC is an important diagnostic tool that can provide valuable information to pathologists. When used along with H&E staining and other special stains, IHC helps identify cell types and origins that can aid in cancer diagnosis, classification, and determining appropriate treatment. Different tumor types express specific protein markers detectable by IHC. While IHC results must be interpreted carefully, they can help diagnose poorly differentiated tumors, identify primary sites of metastatic cancers, and guide personalized cancer treatment decisions. Large antibody panels are used for different cancer types to provide diagnostic, prognostic and predictive information through protein expression profiling.

















































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
















