Downloaded 33 times


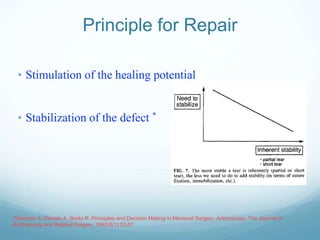

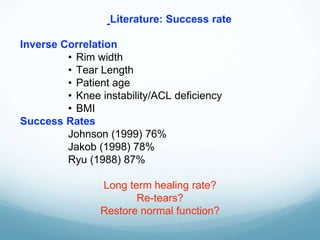
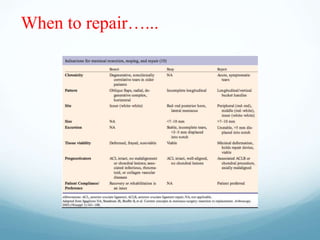
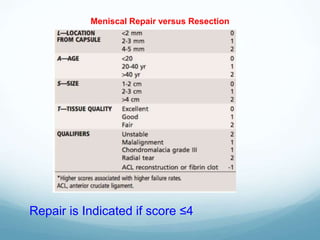



Dr. Rajat Jangir discusses indications for meniscus repair in athletically active patients, emphasizing the importance of restoring function and minimizing contact stress. He notes that not all meniscal tears should be repaired, highlighting the need for informed decision-making, as only 20% are deemed repairable. The document outlines principles for successful repair, including stimulation of healing and stabilization of the defect, while also addressing factors that influence repair success rates.




















































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


