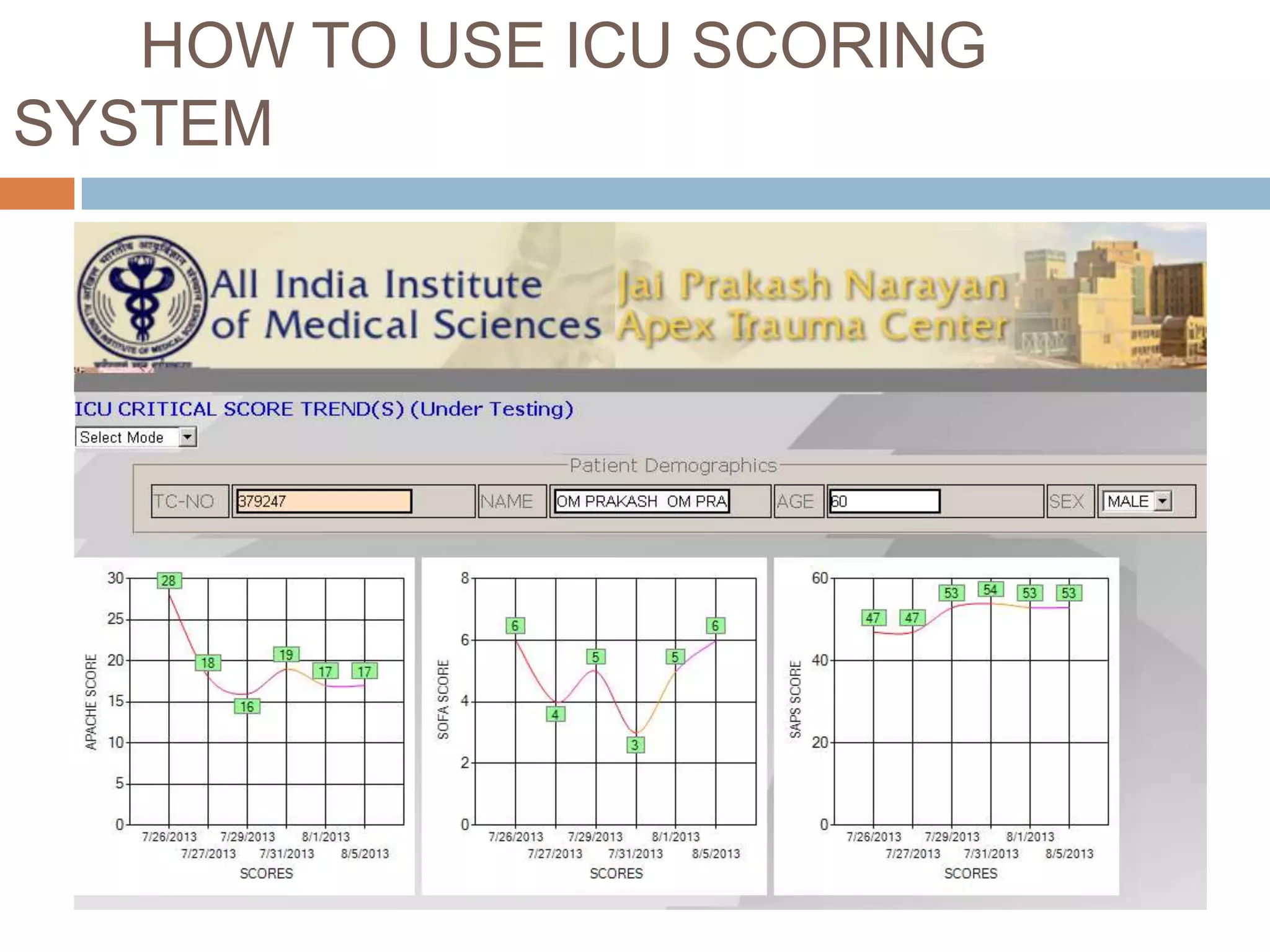
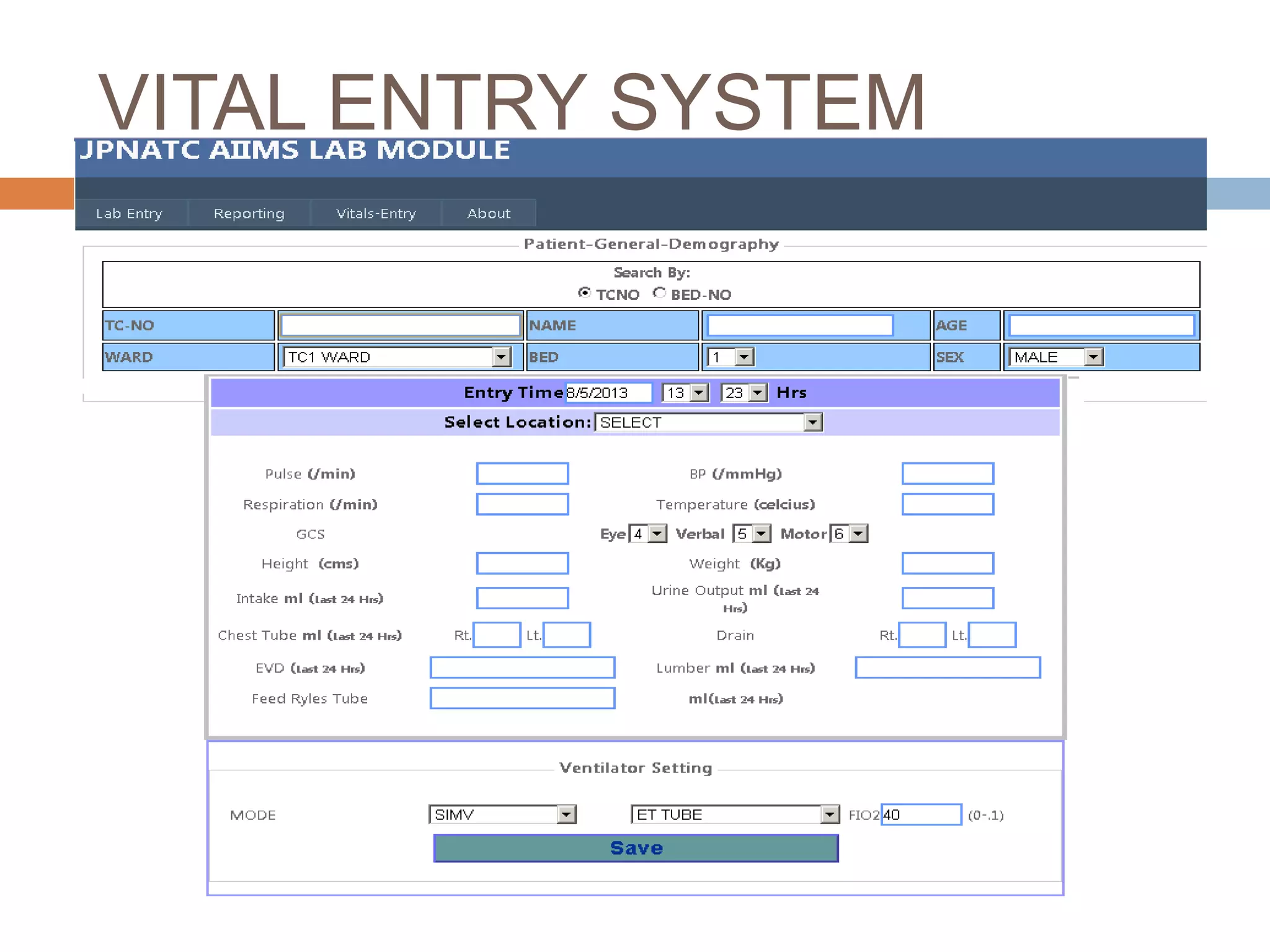


This document describes an ICU scoring system developed at AIIMS to calculate the severity of disease and prognosis of ICU patients. It discusses the different types of ICU scores including APACHE, SOFA, and SAPS. It outlines how the system works, including vital entry, lab modules, and homepage. The roles of nurses in providing training and data entry are highlighted. Benefits include easy assessment, performance comparison, and graphical data representation. Challenges in implementation centered around computer training for nurses. Compliance is reported as 100% in the neuro ICU.





















































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)















