Downloaded 314 times
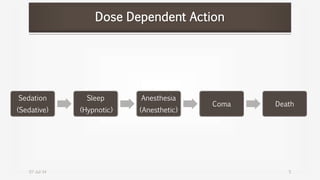
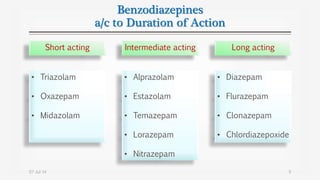
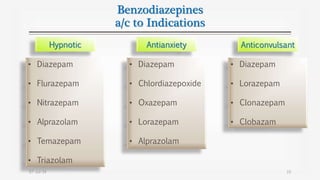
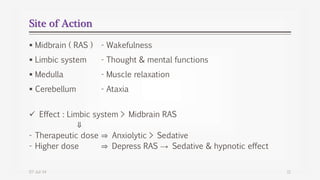

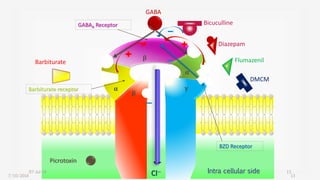
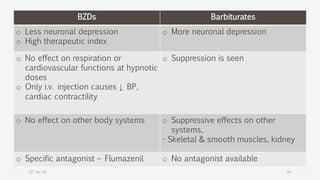
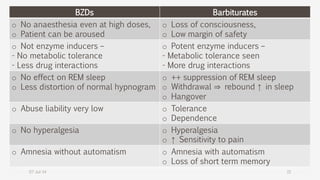
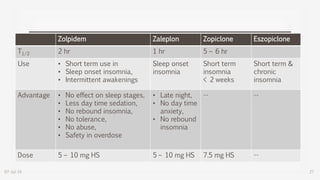
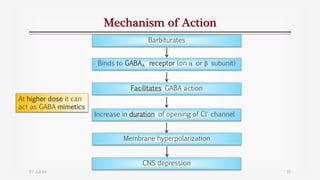

Sedatives and hypnotics are drugs that calm or induce sleep. Common classes include benzodiazepines (BZDs), barbiturates, and non-BZD hypnotics. BZDs are widely used and bind to GABA receptors to facilitate the effects of GABA, producing sedation, hypnosis, or anesthesia in a dose-dependent manner. They have a high safety profile but can cause dependence. Barbiturates also act at GABA receptors but have a lower safety margin and greater risk of overdose. Newer non-BZD drugs like zolpidem, zaleplon, and zopiclone have fewer side effects and lower abuse potential than B





















































![4._Sedative_hypnotics[1].pptx pharmacy students](https://cdn.slidesharecdn.com/ss_thumbnails/4-251117163021-acac7ad2-thumbnail.jpg?width=640&height=640&fit=bounds)






































