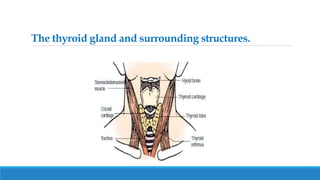
The thyroid gland is located in the lower neck and produces thyroid hormones that regulate metabolism. Hyperthyroidism occurs when the thyroid gland is overactive and produces excessive thyroid hormones. Graves' disease is the most common cause of hyperthyroidism and results in symptoms like nervousness, rapid heartbeat, weight loss, and bulging eyes. Treatment options for hyperthyroidism include radioactive iodine therapy which destroys the thyroid gland, anti-thyroid medications that reduce hormone production, or surgery to remove part of the thyroid gland.