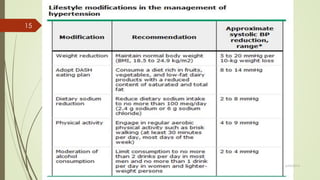
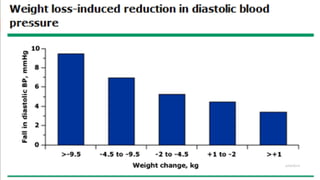
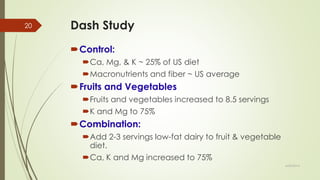
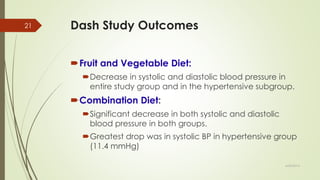
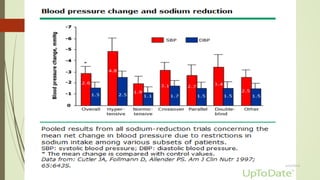
This document discusses non-pharmacologic management of hypertension. It recommends lifestyle modifications including weight loss, following the DASH diet which emphasizes fruits/vegetables, reducing sodium intake, regular exercise, limiting alcohol, and patient education. Other non-drug therapies mentioned are vitamin D and potassium supplementation, smoking cessation, and limiting NSAIDs and acetaminophen. The DASH diet was shown to lower blood pressure comparable to medication, especially when combined with low-fat dairy.