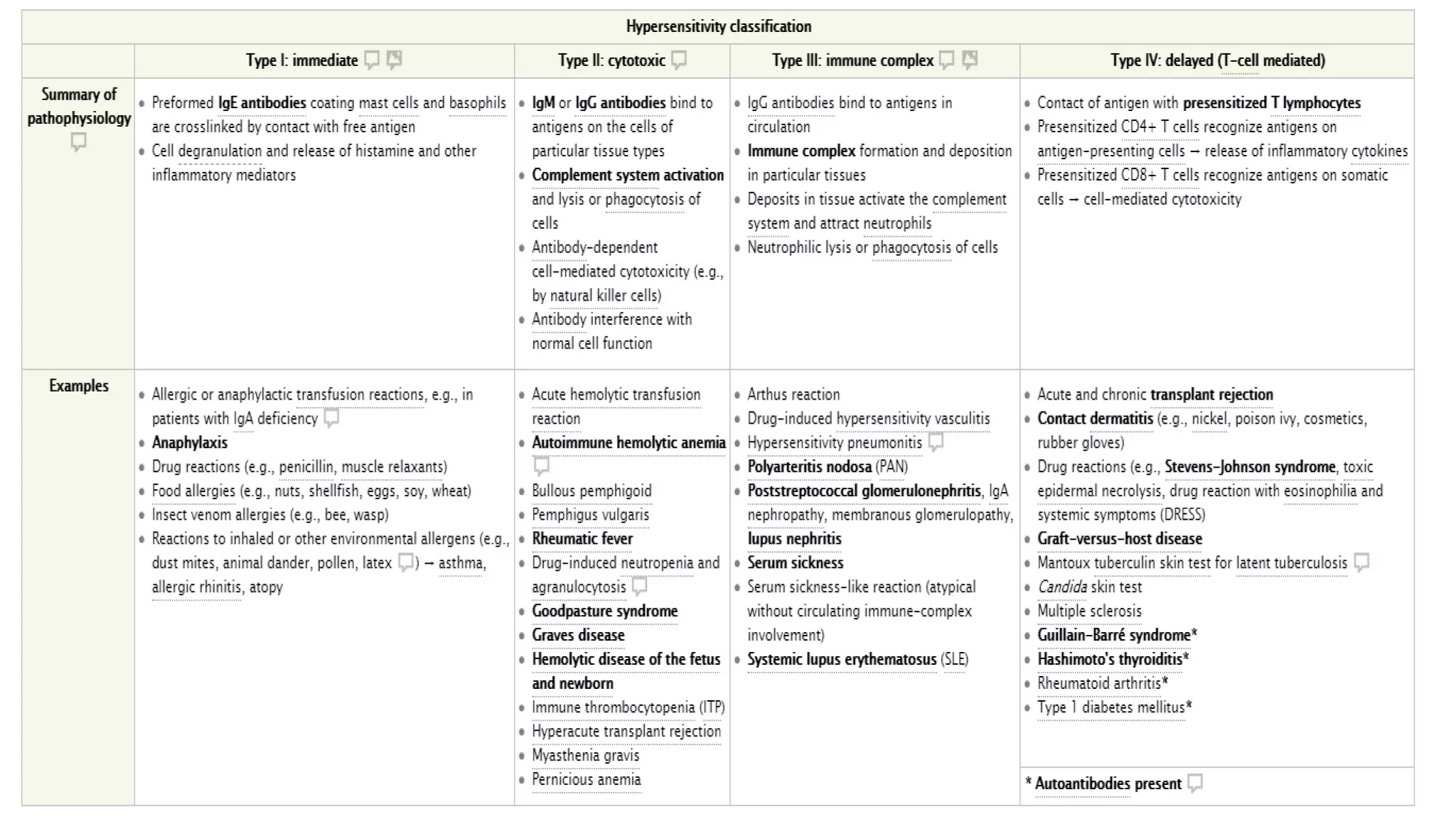
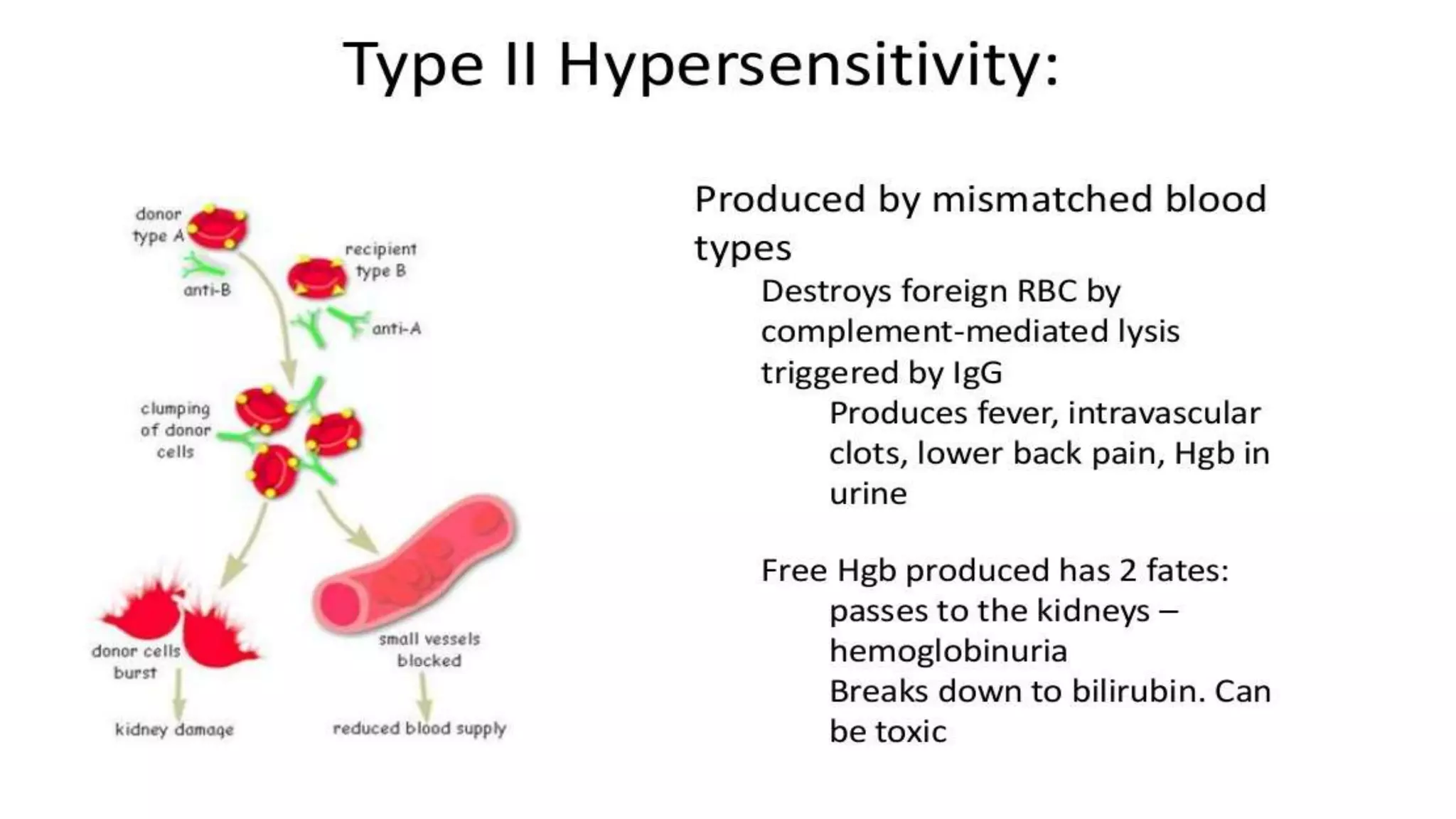
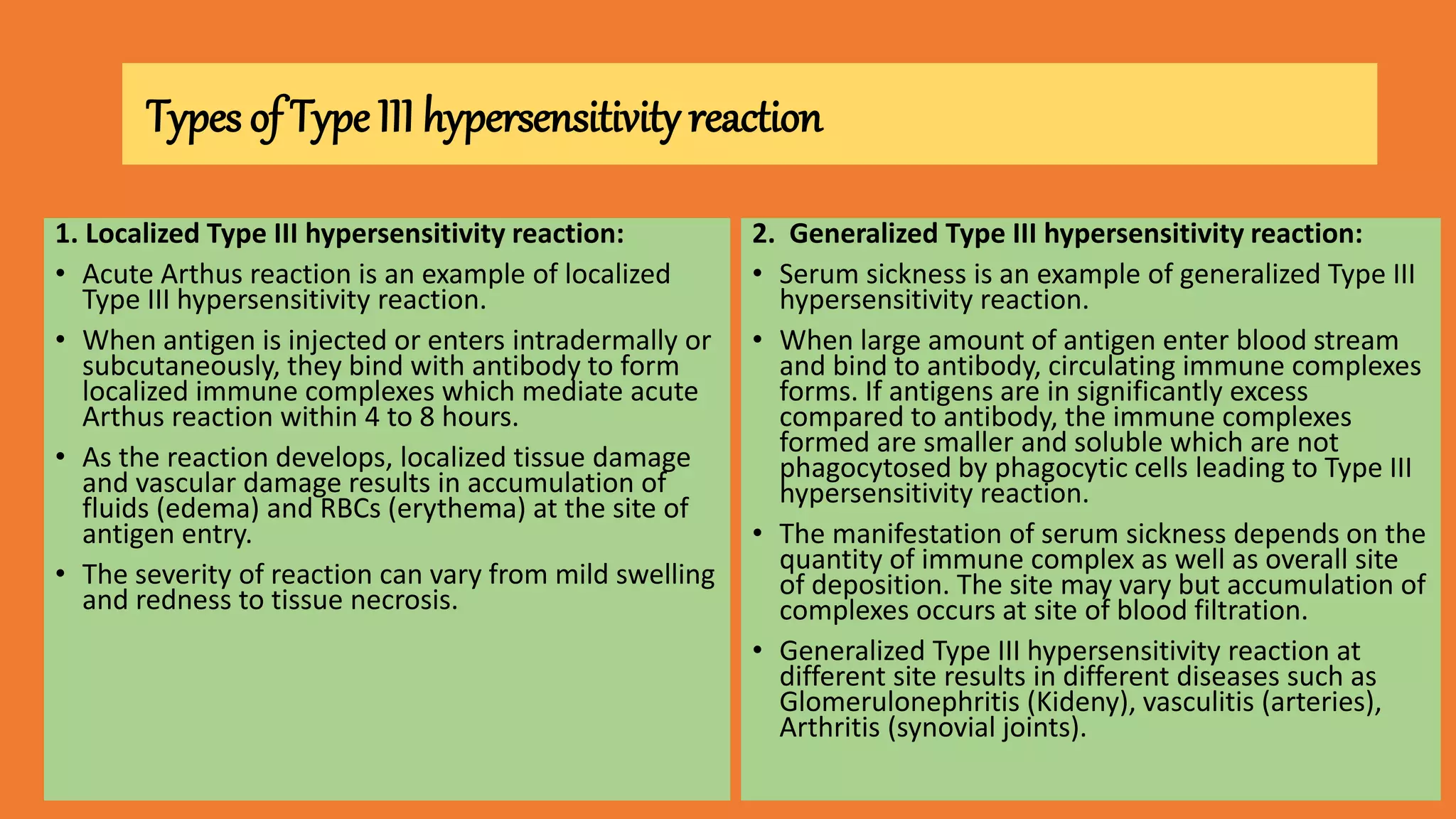
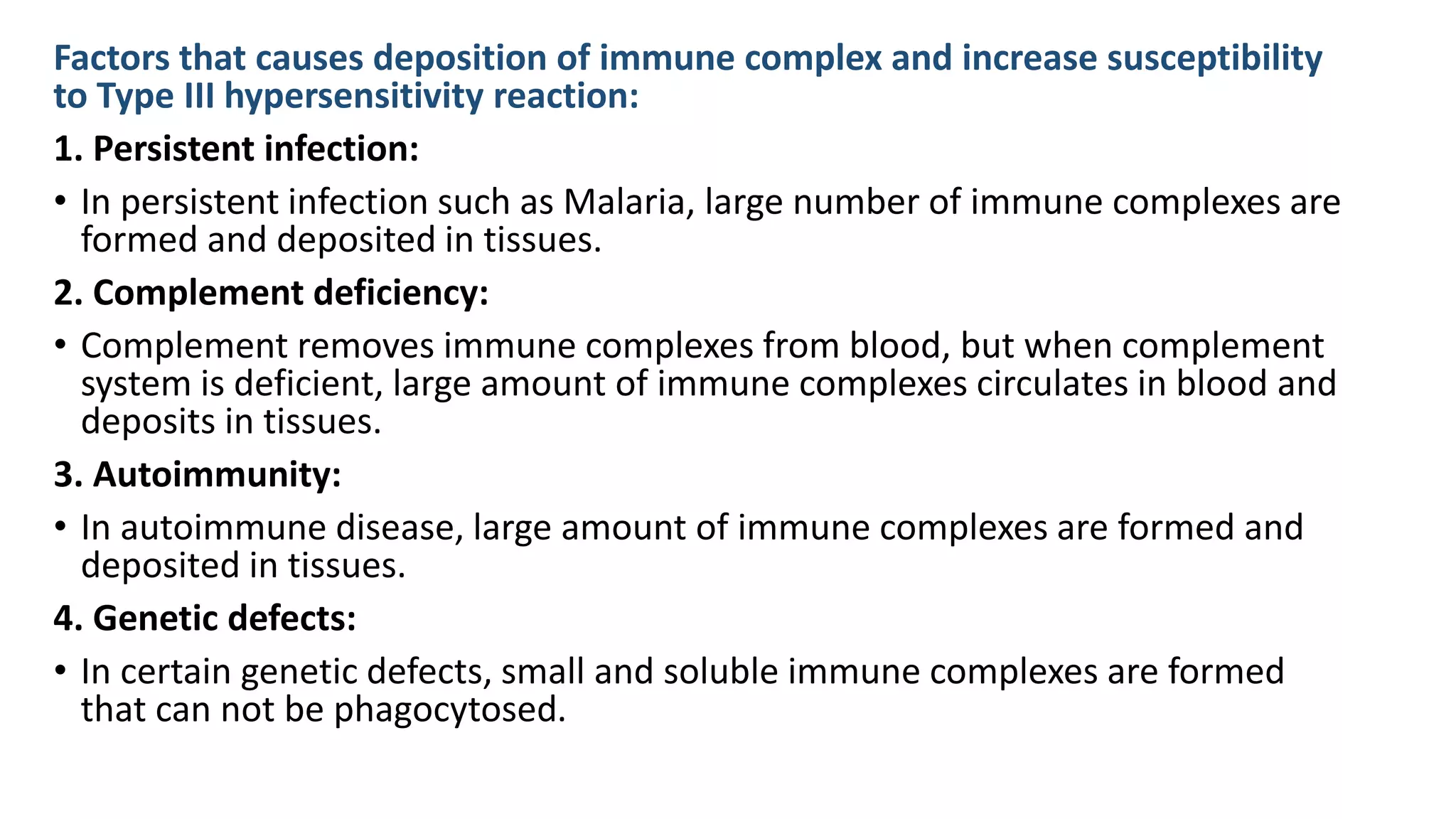
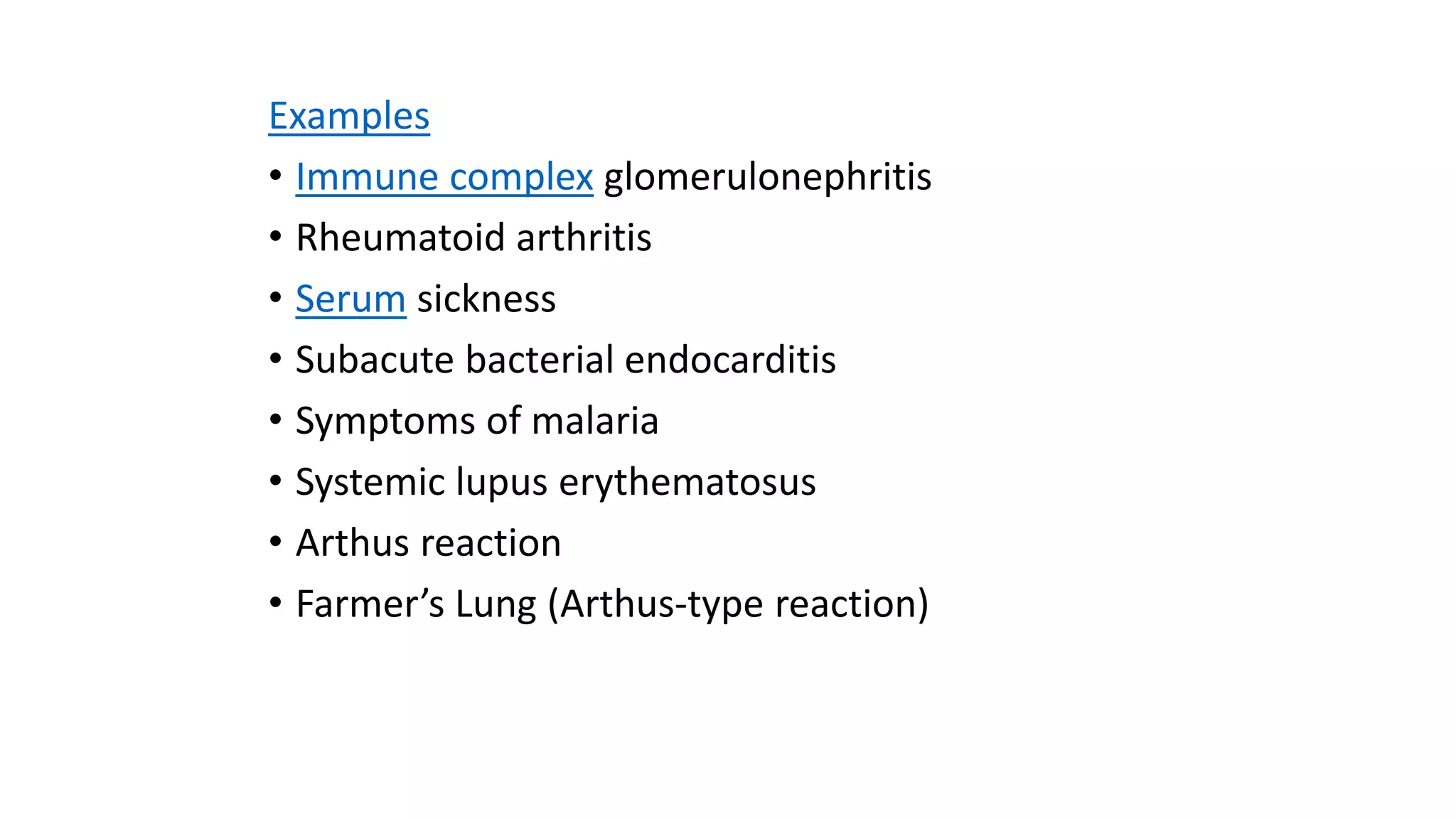
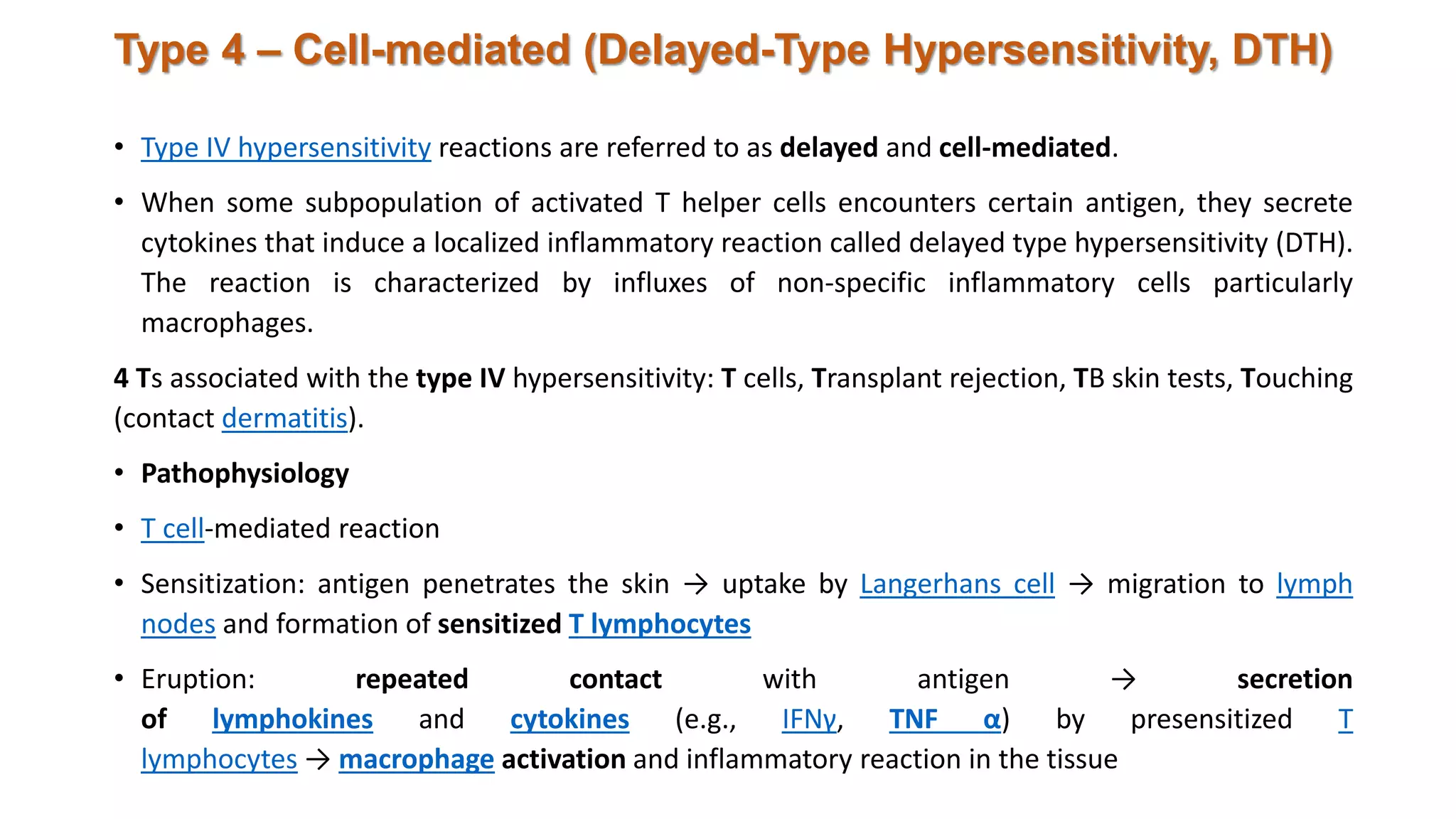
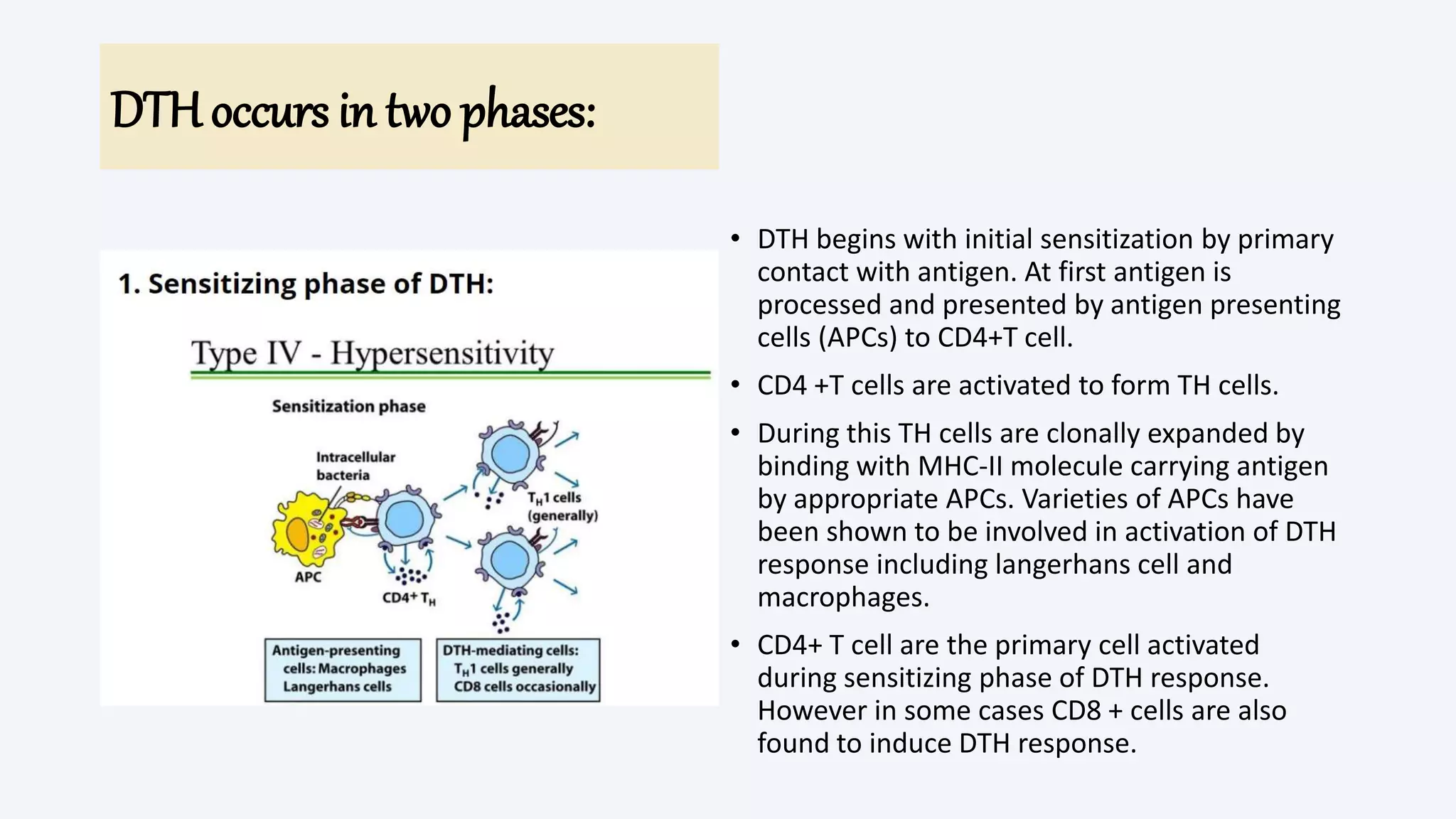
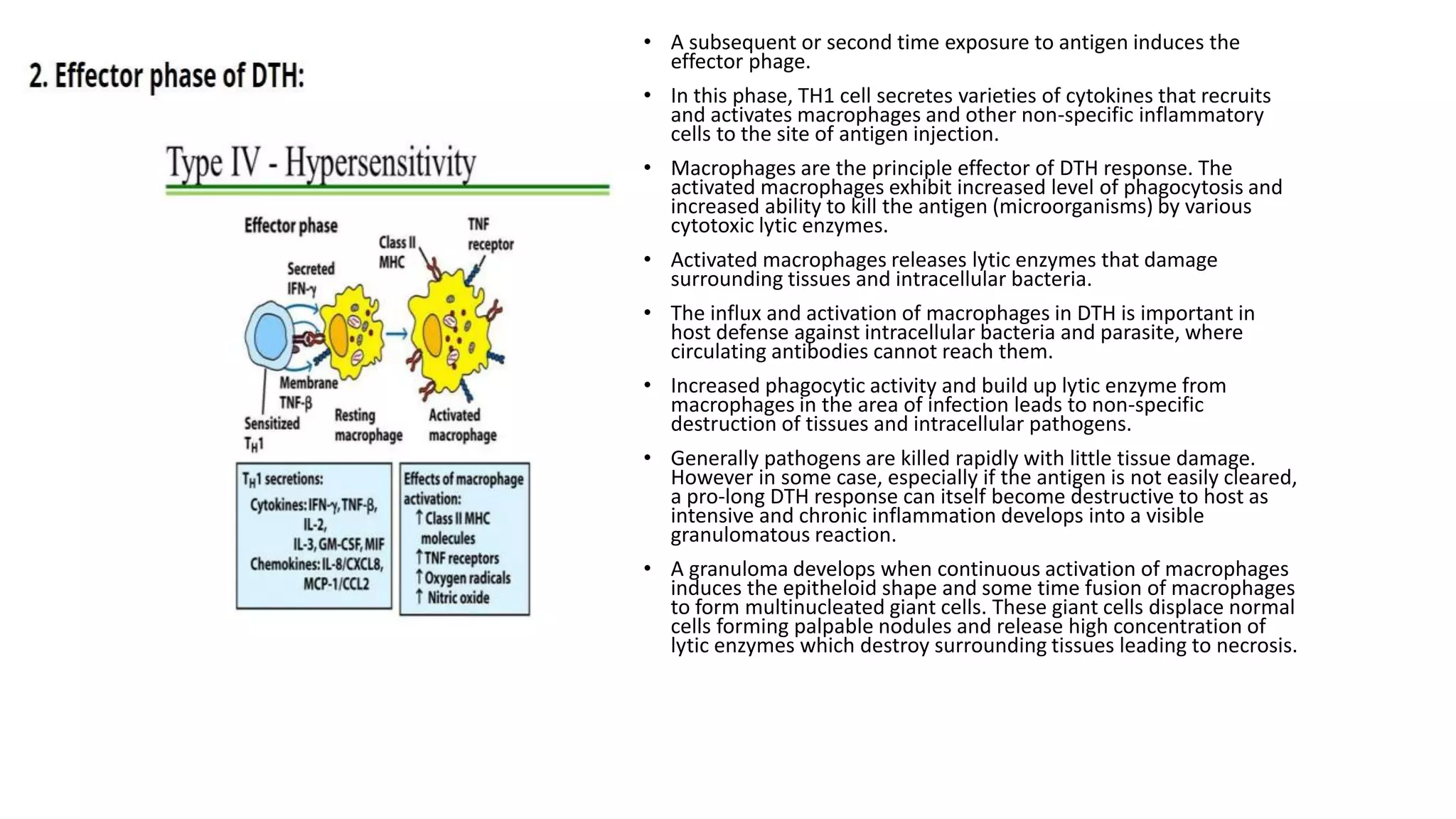
The document discusses hypersensitivity reactions, which are harmful immune responses to typically harmless antigens, classifying them into four types: Type I (immediate), Type II (cytotoxic), Type III (immune complex), and Type IV (cell-mediated). Each type has distinct clinical features, diagnostic methods, and treatment approaches, with Type I offering symptoms like anaphylaxis and requiring fast intervention, while Type IV involves delayed reactions primarily mediated by T cells. The text outlines associated conditions, testing methods, and treatment strategies for various allergic and autoimmune reactions.





![[Micro] syphilis](https://cdn.slidesharecdn.com/ss_thumbnails/loot4qpwrfcwmtl9jo3e-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190755-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)






























































