The document details the claims process and requirements for various government health programs including Medicare, Champus, and Medicaid, emphasizing the need for accurate information to avoid penalties. It discusses patient authorization for information release, provider-certification of services, and legal consequences for false representations. Additionally, it outlines administrative procedures for handling patient data related to health benefits and eligibility verification.



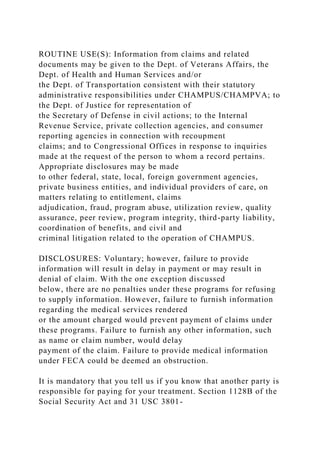


![(101) 111-9685
Female
05-07-1965
Unemployed
]atient status I Married I Divorced
Diagnosis
SPECIAL NOTES:
Case Study
Npl.. 3456789012
INSURANCE INFORMATION:
Patient Number; 2 -11
Place of service: office
Primary Insurance plan: Medicaid
PrlmarylnsuranceplanlD#. 11347765
Group #:
Primary policyholder: sel f
Policyholder Date of Birth.
RelatLonship to Patient.](https://image.slidesharecdn.com/http1500cms-221015083553-16b35067/85/http1500cms-comBECAUSE-THIS-FORM-IS-USED-BY-VARIOUS-docx-10-320.jpg)
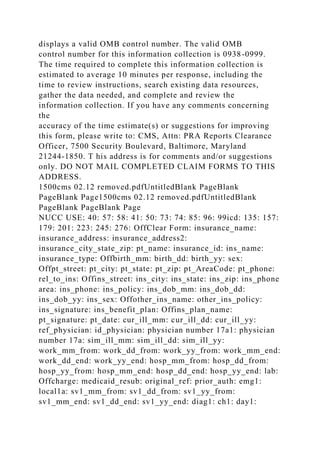
![0: NAD. Sinuses are tender about the maxillary and
frontal areas. TMs, gray
bilaterally. Pharynx is injec.ted, and there ls obvious
purulent material
in the left posterior pharymt. Neck: Supple, no nodes.
Chest: Clear.
COR: RRR without murmur. Lab: Sinus films normal.
A: Clinical chronic sinusitis; her sore throat is probably
from this, but
will obtain a strep test to rule out that possibility, at her
request.
P: Beconase nasal spray, 1 whiff to each nostril q.i.d.
for 1 week, then 1
whiff b.i.d. to each nostril. If she has not improved in 3
weeks, refer
to ENT specialist.
Jleape.eaAha,M.3i.
Henry C. Cardiac, M.D.
(sis; tj''i=ri|niD[i ti`=JLj,k fs`|=ET'i]` I ri - -`y ` `
CASE STUDY 2-7
Fp?o9d?rMstFe?t`?'A¥:,h€rt:Nt:2345. (ioi) 111.2222
Case study
Npl: 3345678901
PROVIDER(S): HENRY C. CARDIAC, M.D. EIN. 22-
1234567 Npl: 3456789012](https://image.slidesharecdn.com/http1500cms-221015083553-16b35067/85/http1500cms-comBECAUSE-THIS-FORM-IS-USED-BY-VARIOUS-docx-12-320.jpg)