


















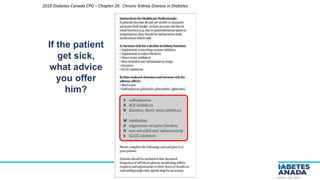






No, the combination of an ACE inhibitor and an ARB is not generally recommended for patients with diabetes and CKD. Some key points: - There is no evidence that combining an ACEi with an ARB provides additional renal protection compared to monotherapy in patients with diabetes and CKD. - Combining the two classes of drugs increases the risk of hyperkalemia and acute kidney injury without proven additional benefit over monotherapy. - Current guidelines recommend using either an ACEi or an ARB as first-line therapy for albuminuria, but do not recommend combining the two classes of drugs. So in summary, while ACEis and ARBs are both reasonable first-line options, combining




































![Presentation T2D_W_Declining_Kidney_Function[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/astrazencapresentationdiatunemshalat2dwdecliningkidneyfunction1-250202101652-511188f8-thumbnail.jpg?width=640&height=640&fit=bounds)


















































