
Recommended
Recommended
More Related Content
Similar to download-key-lessons-on-ldl-c-and-cv-risk.pptx
Similar to download-key-lessons-on-ldl-c-and-cv-risk.pptx (20)
More from UmaShanksr
More from UmaShanksr (17)
Recently uploaded
Recently uploaded (20)
download-key-lessons-on-ldl-c-and-cv-risk.pptx
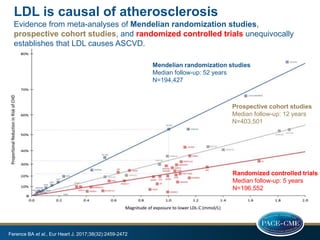
- 1. LDL is causal of atherosclerosis Evidence from meta-analyses of Mendelian randomization studies, prospective cohort studies, and randomized controlled trials unequivocally establishes that LDL causes ASCVD. Ference BA et al., Eur Heart J. 2017;38(32):2459-2472 Mendelian randomization studies Median follow-up: 52 years N=194,427 Prospective cohort studies Median follow-up: 12 years N=403,501 Randomized controlled trials Median follow-up: 5 years N=196,552
- 2. LDL-c level increases with age, so does the risk of atherogenesis 2.0 3.0 4.0 5.0 6.0 1 3 5 7 9 11 13 LDL-c cholesterol (mmol/l) 7 17 27 37 47 57 67 Age (years) LDL-c rise with age Polygenic hypercholes- terolemia Familial Hypercholes- terolemia Integrated LDL-c exposure Fatty streaks Complex plaque T1 T2 Transitioning pathology Packard CJ. Trends Cardiovasc Med. 2018 Jul;28(5):348-354
- 3. The atherosclerosis disease process changes with time and LDL-c level, and treatment effect depends on the disease phase 2.0 3.0 4.0 5.0 6.0 1 3 5 7 9 11 13 LDL-c cholesterol (mmol/l) 7 17 27 37 47 57 67 Age (years) LDLc rise with age Polygenic hyperchole s-terolemia Familial Hypercholes- terolemia Integrated LDL-c exposure Response to initiation of LDL-c lowering Greater RRR per mmol/l reduction Plaque resolution Lesser RRR Plaque stabilisation Fatty streaks Complex plaque T1 T2 Transitioning pathology Packard CJ. Trends Cardiovasc Med. 2018 Jul;28(5):348-354
- 4. Regression of atherosclerotic plaque is possible with adequate lipid-lowering therapy No significant change from baseline; TAV: Total atheroma volume, PAV: percent atheroma volume 2.7* Prava- statin Significant atherosclerotic progression from baseline -0.4 † † Atorva- statin No significant change from baseline; atherosclerotic progression stopped Change in TAV (%) -1 0 1 2 3 P=0.02 Nissen SE et al. JAMA. 2004 Mar 3;291(9):1071-80, Nicholls SJ et al. JAMA. 2016;316:2373-2384. . Statin monotherapy Statin + evolocumab Significant atherosclerotic regression baseline GLAGOV study 0.05 -0.95 -1.2 -1 -0.8 -0.6 -0.4 -0.2 0 0.2 Change in PAV (%) P < 0.0001 P = NS
- 5. Side effects are not the effect of LDL-c lowering Data of patients with low LDL-c levels at baseline 0.6 0.8 1 1.2 1.4 1.6 Risk ratio in meta-analysis (95%CI) Safety outcomes in non-statin lipid-lowering trials, Experimental vs. control arm Baseline LDL-c <1.8 mmol/L Sabatine MS et al., JAMA Cardiol. 2018;3(9):823-828 Any serious adverse event Aminotrans- ferase elevation New-onset diabetes Hemorrhagic stroke Myalgias or myopathy Cancer
- 6. Side effects are not the effect of achieved LDL-c level 0 0.5 1 1.5 2 2.5 3 3.5 4 4.5 Adjusted OR (95%CI) Safety of achieving very low LDL-c with PCSK9 inhibition (FOURIER trial, evolocumab) <0.5 mmol/L 0.5 - <1.3 mmol/L 1.3 - <1.8 mmol/L 1.8 to <2.6 mmol/L >2.6 mmol/L (reference) P-trend: 0.30 0.13 0.64 0.72 0.15 0.48 0.43 0.72 0.91 0.73 Giuliano RP et al., Lancet. 2017;390(10106):1962-1971 Serious adverse events New or progressive malignancy Cataract- related adverse events New onset diabetes mellitus Stopping study drug due to AE Neuro- cognitive events AST / ALT >3x ULN Creatine kinase >5x ULN Haemo rrhagic stroke Non-CV death Achieved LDL-c
- 7. Lowering LDL-c to very low levels is safe Exploratory analysis in FOURIER trial 0 5 10 15 20 25 Serious AE Stopping study drug due to AE Incidence (%) Safety outcomes at 4 weeks N=504, median [IQR] LDL-c: 0.18 [0.13-0.23] mM, 7 [5-9] mg/dL >2.6 mM <0.26 mM (<10 mg/dL) HR: 0.94 (95%CI: 0.74-1.20) P=0.61 HR: 1.08 (95%CI: 0.63-1.85) P=0.78 Giuliano RP et al., Lancet. 2017;390(10106):1962-1971
- 8. Use combination therapy for additive LDL-c lowering effect to reduce CV risk IMPROVE-IT: ezetimibe + simvastatin vs. simvastatin, after ACS Primary endpoint: CV death, MI, unstable angina requiring hospitalization, coronary revascularization (≥30 days), stroke. Median follow-up: 6 years HR: 0.936 (95%CI: 0.89-0.99), P=0.016 FOURIER trial: evolocumab vs. placebo, plus background statin therapy after ACS Primary endpoint: CV death, MI, stroke, hospitalization for unstable angina, or coronary revascularization. Median follow-up: 2.2 years HR: 0.85 (95%CI: 0.79-0.99), P<0.001 ODYSSEY OUTCOMES trial: alirocumab vs placebo, on top of high-intensity statin therapy, after ACS Primary endpoint: death from coronary heart disease, nonfatal MI, fatal or nonfatal ischemic stroke, or unstable angina requiring hospitalization. Median follow-up: 2.8 years HR: 0.85 (95%CI: 0.78-0.93), P<0.001 Cannon CP et al., N Engl J Med. 2015;372(25):2387-97, Sabatine MS et al., New Engl J Med 2017;376:1713, Schwartz et al., N Engl J Med. 2018;379(22):2097-2107.
- 9. Even below LDL-c target further LDL-c reduction gives additional CV benefit A quarter of a century of treating LDL-C 0 20 40 60 80 100 120 140 160 180 200 High is bad Average is not good Lower is better Even lower is even better Lowest is best 1994 1996-2002 2004-2005 2015 2017 TNT mg/dL
- 10. Even below LDL-c target further LDL-c reduction gives additional CV benefit 1,00 0.71 0.64 0.58 0.56 0.51 0.44 0 0.2 0.4 0.6 0.8 1 >175 150 - 175 125 - 150 100 - 125 75 - 100 50 - 75 < 50 adjusted HR (95%CI)* > 4.52 3.88 - 4.52 3.23 - 3.88 2.58 - 3.23 1.94 - 2.58 1.29 - 1.94 < 1.29 (0,53-0,79) (0,48-0,69) (0,46-0,67) (0,42-0,62) (0,35-0,55) mg/dL mmol/L (Ref.) (0,56-0,89) Risk for Major CV Events by Achieved on-Trial LDL-C levels Boekholdt et al. JACC 2014; 64: 485-494 * Adjusted for sex, age, smoking status, presence of DM, SBP, HDL-C and trial
- 11. Even below LDL-c target further LDL-c reduction gives additional CV benefit Exploratory analysis in FOURIER trial in those with very low LDL-c 0 2 4 6 8 10 12 14 CV death, MI, stroke, UA, coron. Revasc CV death, MI, stroke Incidence (%) Efficacy outcomes at 4 weeks N=504, median [IQR] LDL-c: 0.18 [0.13-0.23] mM, 7 [5-9] mg/dL >2.6 mM <0.26 mM (<10 mg/dL) HR: 0,69 (95%CI: 0.49-0.79) P=0.03 HR: 0,59 (95%CI: 0.37-0.92) P=0.02 Giuliano RP et al., Lancet. 2017;390(10106):1962-1971
- 12. Greatest risk reduction can be achieved in the highest risk groups 0 50 100 150 200 250 300 70 mg/dL 100 mg/dL 130 mg/dL 160 mg/dL 190 mg/dL NNT 5-year number needed to treat (NNT) Max. statin therapy + ezetimibe: 20% LDL-c reduction Very high risk (>30% 10-yr ASCVD risk) High risk (20% -30% 10-yr ASCVD risk) Moderate risk (10% -20% 10-yr ASCVD risk) Robinson JG et al., J Am Coll Cardiol. 2016;68(22):2412-2421 0 50 100 150 200 250 300 70 mg/dL 100 mg/dL 130 mg/dL 160 mg/dL 190 mg/dL NNT 5-year number needed to treat (NNT) Max. statin therapy + PCSK9 mAb: 50% LDL-c reduction Very high risk (>30% 10-yr ASCVD risk) High risk (20% -30% 10-yr ASCVD risk) Moderate risk (10% -20% 10-yr ASCVD risk)
- 13. Statin therapy is remarkably safe Mach F et al., Eur Heart J. 2018;39(27):2526-2539, Collins R et al., Lancet. 2016; 388(10059):2532-2561 NO evidence to support adverse effects of statins on: Cognitive function, clinically significant renal deterioration, risk of cataract and risk of haemorrhagic stroke in patients without prior stroke Typically, treating 10.000 patients for 5 years with a standard statin regimen, is expected to prevent: 1000 major vascular events (secondary prevention) 500 major vascular events (primary prevention) to cause: 5 cases of myopathy 50-100 new cases of diabetes 5-10 hemorrhagic strokes (in those with prior stroke) 50-100 patients may experience symptomatic adverse events such as muscle pain or weakness. Placebo-controlled randomized trials show that almost all of these cases are misattributed.
- 14. When statin therapy is discontinued, the risk of CV events and mortality increases Danish study: 2.176.361 person-years (median FU: 4.3 years, range: 0-14) Cumulative incidence of events from 6 months after initiation of statin therapy in individuals with early statin discontinuation vs. those with continued use Discontinuation: no second dispense in first 6 months after initiation 424.000 who continued statin were matched 5:1 with 84.800 who discontinued. Myocardial infarction: After 10 years: 9.9 vs. 8.0%, adjusted HR: 1.26 (95%CI: 1.21-1.30) Death from CV disease: After 10 years: 10.6 vs. 9.5%, adjusted HR: 1.18 (95%CI: 1.14-1.23) Nielsen SF and Nordestgaard BG. Eur Heart J. 2016;37(11):908-916 0 2 4 6 8 10 12 MI CV death Cumulative incidence (%) 10 years after statin initiation Discontinuation Continued use
- 15. After an event, initiate the right treatment in hospital EUROASPIRE IV data showed that a large majority of coronary patients do not achieve the guideline standards for secondary prevention, regarding lifestyle, risk factor and therapeutic management. Dutch single-center observational registry (>9000 patients with ACS) studied ACS care between 2006 and 2014 Optimal medical therapy (OMT): aspirin, P2Y12 inhibitors, statin, beta-blockers, and ACEi/ARB , Kotseva K et al., Eur J Prev Cardiol. 2016;23(6):636-48, Hoedemaker NPG et al., Eur Heart J Cardiovasc Pharmacother. 2018;4(2):102-110 0 2 4 6 8 10 Crude Kaplan-Meier 1-year mortality rates (%) All-cause mortality in survivors of the index hospitalization No OMT at discharge OMT at discharge OMT vs. no-OMT Unadjusted HR : 0.35, 95%CI: 0.28-0.44 Adjusted HR: 0.66, 95%CI: 0.46-0.93 (Adjusted for age, gender, diagnosis STEMI, preadmission medication, diabetes, hypertension, previous MI, previous stroke, shock during acute phase, eGFR <60 mL/min/1.73 m2, PCI during hospitalization, OAC at discharge, SBP at discharge, and heart rate at discharge.)
- 16. LDL-c lowering treatment impacts disease progression before clinical manifestation Robinson JG et al., J Am Heart Assoc. 2018 Oct 16;7(20):e009778 Life course trajectory of atherosclerotic progression for different CV risk categories and the hypothesized effects of intensive LDL-c lowering.
- 17. Screening for familial hypercholesterolemia after ACS pays off 0 2 4 6 8 10 Adjusted HR (95%CI) Risks of recurrent events after ACS, Per Dutch Lipid Clinic Definition Category No FH Possible FH Probable/definite FH Coronary events Cardiovascular events Nanchen D et al., Circulation. 2016;134(10):698-709 Patients with FH and ACS have a >2-fold adjusted risk of coronary event recurrence within the first year after discharge, as compared with those without FH.
Editor's Notes
- Adjusted for traditional cardiovascular risk factors, including age, sex, body mass index, current smoking, hypertension, and diabetes mellitus, as well as high-intensity statins at discharge and attendance at cardiac rehabilitation.