How I Think, How I Treat: BTK Inhibitors as a Clinical Strategy in CLL, MCL, and Beyond—Therapeutic Selection, Sequencing, and Next Steps.
•
0 likes•60 views

Andre H. Goy, MD, Richard R. Furman, MD, Krish Patel, MD, and Deborah M. Stephens, DO, prepared useful practice aids pertaining to B-cell malignancies for this CME activity titled "How I Think, How I Treat: BTK Inhibitors as a Clinical Strategy in CLL, MCL, and Beyond—Therapeutic Selection, Sequencing, and Next Steps." For the full presentation, monograph, complete CME information, and to apply for credit, please visit us at http://bit.ly/2P5FeQk. CME credit will be available until December 29, 2020.

Recommended
Recommended
More Related Content
What's hot
What's hot (18)
Similar to How I Think, How I Treat: BTK Inhibitors as a Clinical Strategy in CLL, MCL, and Beyond—Therapeutic Selection, Sequencing, and Next Steps.
Similar to How I Think, How I Treat: BTK Inhibitors as a Clinical Strategy in CLL, MCL, and Beyond—Therapeutic Selection, Sequencing, and Next Steps. (20)
More from PVI, PeerView Institute for Medical Education
More from PVI, PeerView Institute for Medical Education (20)
Recently uploaded
Recently uploaded (20)
How I Think, How I Treat: BTK Inhibitors as a Clinical Strategy in CLL, MCL, and Beyond—Therapeutic Selection, Sequencing, and Next Steps.
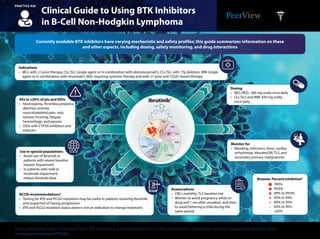
- 1. Clinical Guide to Using BTK Inhibitors in B-Cell Non-Hodgkin Lymphoma PRACTICE AID Access the activity,“How I Think, How I Treat: BTK Inhibitors as a Clinical Strategy in CLL, MCL, and Beyond—Therapeutic Selection, Sequencing, and Next Steps,” at www.peerview.com/FKM40. AEs in ≥20% of pts and DDIs • Neutropenia, thrombocytopenia, diarrhea, anemia, musculoskeletal pain, rash, nausea, bruising, fatigue, hemorrhage, and pyrexia • DDIs with CYP3A inhibitors and inducers Use in special populations • Avoid use of ibrutinib in patients with severe baseline hepatic impairment • In patients with mild or moderate impairment, reduce ibrutinib dose Dosing • MCL/MZL: 560 mg orally once daily • CLL/SLL and WM: 420 mg orally once daily Monitor for • Bleeding, infections, fever, cardiac arrhythmias, elevated BP, TLS, and secondary primary malignancies Assess/advise • CBCs monthly; TLS baseline risk • Women to avoid pregnancy while on drug and 1 mo after cessation, and men to avoid fathering a child during the same period Kinome: Percent Inhibition5 NCCN recommendations4 • Testing for BTK and PLCG2 mutations may be useful in patients receiving ibrutinib and suspected of having progression • BTK and PLCG2 mutation status alone is not an indication to change treatment Indications • MCL with ≥1 prior therapy, CLL/SLL (single agent or in combination with obinutuzumab2 ), CLL/SLL with 17p deletion, WM (single agent or in combination with rituximab3 ), MZL requiring systemic therapy and with ≥1 prior anti-CD20–based therapy Currently available BTK inhibitors have varying mechanistic and safety profiles; this guide summarizes information on these and other aspects, including dosing, safety monitoring, and drug interactions Ibrutinib1 TKL STE CK1 AGC CAMKCMGC Other TK N N N N N H2 N O O 100% 99.9% 99% to 99.9% 95% to 99% 90% to 95% 65% to 90% <65%
- 2. Clinical Guide to Using BTK Inhibitors in B-Cell Non-Hodgkin Lymphoma PRACTICE AID Access the activity,“How I Think, How I Treat: BTK Inhibitors as a Clinical Strategy in CLL, MCL, and Beyond—Therapeutic Selection, Sequencing, and Next Steps,” at www.peerview.com/FKM40. AEs in ≥20% of pts and DDIs • Neutropenia, thrombocytopenia, diarrhea, anemia, musculoskeletal pain, rash, nausea, bruising, fatigue, hemorrhage, and pyrexia • DDIs with CYP3A inhibitors and inducers, and gastric acid–reducing agents (PPIs, H2-receptor antagonists, and antacids) Use in special populations • Advise women not to breastfeed Dosing • 100 mg orally approximately every 12 h; swallow whole with water, with or without food • Advise not to break, open, or chew capsule Monitor for • Bleeding, signs and symptoms of infections, secondary primary malignancies, atrial fibrillation, and trial flutter Assess/advise • CBCs monthly • Patients to use sun protection Kinome: Percent Inhibition5 NCCN recommendations4 • NCCN also recommends acalabrutinib for relapsed/refractory CLL (except ibrutinib-refractory CLL with BTK C481S mutations) • Patients with ibrutinib intolerance have been successfully treated with acalabrutinib without recurrence of these symptoms Indications • Adult patients with MCL who have received ≥1 prior therapy Currently available BTK inhibitors have varying mechanistic and safety profiles; this guide summarizes information on these and other aspects, including dosing, safety monitoring, and drug interactions Acalabrutinib6 TKL STE CK1 AGC CAMKCMGC Other TK O N N N NH2 N O NH N 100% 99.9% 99% to 99.9% 95% to 99% 90% to 95% 65% to 90% <65%
- 3. AE: adverse event; BTK: Bruton's tyrosine kinase; CAMK: calcium/calmodulin-dependent protein kinase; CBC: complete blood count; CK1: casein kinase 1; CLL: chronic lymphocytic leukemia; CYP3A: cytochrome P450 3A; DDI: drug–drug interaction; MCL: mantle cell lymphoma; MZL: marginal zone B-cell lymphoma; NCCN: National Comprehensive Cancer Network; PPI: proton pump inhibitor; SLL: small lymphocytic lymphoma; STE: sulfotransferase, estrogen-preferring; TK: tyrosine kinase; TKL: tyrosine kinase–like; TLS: tumor lysis syndrome; WM: Waldenström’s macroglobulinemia. 1. Imbruvica (ibrutinib) Prescribing Information. https://www.accessdata.fda.gov/drugsatfda_docs/label/2015/205552s002lbl.pdf. Accessed November 12, 2019. 2. http://www.ascopost.com/News/59690. Accessed November 12, 2019. 3. http://www.ascopost.com/News/59204. Accessed November 12, 2019. 4. NCCN Clinical Practice Guidelines in Oncology. Chronic Lymphocytic Leukemia/Small Lymphocytic Lymphoma. Version 2.2020. 5. Kaptein A et al. 60th American Society of Hematology Meeting and Exposition (ASH 2018). Abstract 1871. 6. Calquence (acalabrutinib) Prescribing Information. https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/210259s000lbl.pdf. Accessed November 12, 2019. 7. Brukinsa (zanubrutinib) Prescribing Information. https://www.accessdata.fda.gov/drugsatfda_docs/ label/2019/213217s000lbl.pdf. Accessed November 12, 2019. Clinical Guide to Using BTK Inhibitors in B-Cell Non-Hodgkin Lymphoma PRACTICE AID Access the activity,“How I Think, How I Treat: BTK Inhibitors as a Clinical Strategy in CLL, MCL, and Beyond—Therapeutic Selection, Sequencing, and Next Steps,” at www.peerview.com/FKM40. AEs in ≥20% of pts and DDIs • Neutropenia, thrombocytopenia, upper respiratory tract infection, decreased white blood cells, decreased hemoglobin, rash, bruising, diarrhea, and cough • DDIs with CYP3A inhibitors and inducers Use in special populations • In patients with severe hepatic impairment, reduce zanubrutinib dose • Advise women not to breastfeed Dosing • 160 mg orally twice daily or 320 mg orally once daily; swallow whole with water, with or without food • Advise not to break, open, or chew capsule Monitor for • Bleeding, signs and symptoms of infections, secondary primary malignancies, atrial fibrillation, and atrial flutter Assess/advise • CBCs • Avoid use during pregnancy Indications • Adult patients with MCL who have received ≥1 prior therapy Currently available BTK inhibitors have varying mechanistic and safety profiles; this guide summarizes information on these and other aspects, including dosing, safety monitoring, and drug interactions TKL STE CK1 AGC CAMKCMGC Other TK Zanubrutinib7 N N N HN H2 N O O O Kinome: Percent Inhibition5 100% 99.9% 99% to 99.9% 95% to 99% 90% to 95% 65% to 90% <65%
- 4. Selected Studies With BTK Inhibitors Clinical Trial Landscape of B-Cell Non-Hodgkin Lymphoma1 PRACTICE AID Access the activity,“How I Think, How I Treat: BTK Inhibitors as a Clinical Strategy in CLL, MCL, and Beyond—Therapeutic Selection, Sequencing, and Next Steps,” at www.peerview.com/FKM40. Ibrutinib Zanubrutinib (BGB-3111) Key: ˜ Active, not recruiting ˜ Currently recruiting Phase 3 Clinical Trials Phase 3 Clinical Trials PFS NCT01776840 (SHINE) Ibrutinib + bendamustine + rituximab in patients with newly diagnosed MCL CR, VGPR NCT03053440 (BGB-3111-302 ASPEN) Zanubrutinib vs ibrutinib in patients with WM PFS NCT02947347 (PERSPECTIVE) Ibrutinib + rituximab in patients with treatment-naïve FL PFS NCT03112174 (SYMPATICO) Ibrutinib + venetoclax in previously treated patients with MCL PFS ISRCTN01844152 (FLAIR)2 Ibrutinib monotherapy vs ibrutinib + rituximab vs ibrutinib + venetoclax vs FCR in patients with treatment-naïve CLL/SLL TLS, DLT, PFS, CR NCT03462719 (GLOW/CLL 3011) Ibrutinib + venetoclax vs chlorambucil + obinutuzumab for patients with newly diagnosed CLL/SLL PFS NCT03336333 (BGB-3111-304 SEQUOIA) Zanubrutinib vs bendamustine + rituximab in patients with previously untreated CLL/SLL Approved BTK inhibitors currently include ibrutinib, acalabrutinib, and zanubrutinib Primary Endpoint(s) Primary Endpoint(s)
- 5. BTK: Bruton's tyrosine kinase; CLL: chronic lymphocytic leukemia; CR: complete response; DLT: dose-limiting toxicities; FCR: fludarabine, cyclophosphamide, and rituximab; FL: follicular lymphoma; MCL: mantle cell lymphoma; MRD-CR: minimal residual disease–negative complete response; R/R: relapsed/refractory; SLL: small lymphocytic lymphoma; TLS: tumor lysis syndrome; TN: treatment naïve; VGPR: very good partial response; WM: Waldenström’s macroglobulinemia. 1. https://clinicaltrials.gov/ct2/home. Accessed November 19, 2019. 2. https://www.cancerresearchuk.org/about-cancer/find-a-clinical-trial/a-trial-ibrutinib-rituximab-chronic-lymphocytic-leukaemia-flair#undefined. Accessed November 19, 2019. 3. Sharman JP et al. 61st Annual Meeting & Exposition of the American Society of Hematology (ASH 2019). Abstract 31. 4. NCCN Clinical Practice Guidelines in Oncology. B-Cell Lymphomas. Version 5.2019. https://www.nccn.org/professionals/physician_gls/pdf/b-cell.pdf. Accessed November 19, 2019. Selected Studies With BTK Inhibitors Clinical Trial Landscape of B-Cell Non-Hodgkin Lymphoma1 PRACTICE AID Access the activity,“How I Think, How I Treat: BTK Inhibitors as a Clinical Strategy in CLL, MCL, and Beyond—Therapeutic Selection, Sequencing, and Next Steps,” at www.peerview.com/FKM40. PFS Results available (ASH 2019): Acalabrutinib ± obinutuzumab significantly improved PFS vs obinutuzumab + chlorambucil3 NCT02475681 (Elevate CLL TN) Acalabrutinib monotherapy vs acalabrutinib + obinutuzumab vs obinutuzumab + chlorambucil in patients with previously untreated CLL/SLL PFS NCT02972840 (ACE-LY-308) Acalabrutinib + bendamustine/rituximab vs bendamustine/rituximab in patients with previously untreated MCL PFS NCT02970318 (ACE-CL-309) Acalabrutinib vs investigator's choice of idelalisib + rituximab or bendamustine + rituximab in R/R CLL/SLL MRD- CR, time to first therapy NCT03516617 (Phase 2) Acalabrutinib ± obinutuzumab in patients with early stage CLL/SLL MRD- CR NCT03580928 (AVO; Phase 2) Venetoclax + obinutuzumab + acalabrutinib in patients with newly diagnosed CLL/SLL PFS NCT02477696 (Elevate CLL R/R) Acalabrutinib vs ibrutinib in previously treated patients with high-risk CLL/SLL Key: ˜ Active, not recruiting ˜ Currently recruiting Acalabrutinib Primary Endpoint(s) Approved BTK inhibitors currently include ibrutinib, acalabrutinib, and zanubrutinib Phase 3 Clinical Trials NCCN Recommendation4 The NCCN believes that the best management for any patient with cancer is in a clinical trial. Participation in a clinical trial is especially encouraged.