Building Innovative Treatment Options for Patients With B-Cell Malignancies: Practical Insights on Clinical Evidence and Integration Strategies
•
1 like•82 views

This document provides a quick reference guide summarizing diagnostic components, essential immunophenotyping, essential workup, and recent therapeutic innovations for several B-cell malignancies including follicular lymphoma, chronic lymphocytic leukemia, mantle cell lymphoma, and diffuse large B-cell lymphoma. It highlights new agent classes such as monoclonal antibodies, PI3K inhibitors, BTK inhibitors, Bcl-2 inhibitors, IMiDs, and CAR-T cell therapies that have established roles in the treatment of these cancers. The summary is intended to help healthcare professionals apply this information to the care of their patients.

Recommended
Recommended
More Related Content
What's hot
What's hot (18)
Similar to Building Innovative Treatment Options for Patients With B-Cell Malignancies: Practical Insights on Clinical Evidence and Integration Strategies
Similar to Building Innovative Treatment Options for Patients With B-Cell Malignancies: Practical Insights on Clinical Evidence and Integration Strategies (20)
More from PVI, PeerView Institute for Medical Education
More from PVI, PeerView Institute for Medical Education (20)
Recently uploaded
Recently uploaded (20)
Building Innovative Treatment Options for Patients With B-Cell Malignancies: Practical Insights on Clinical Evidence and Integration Strategies
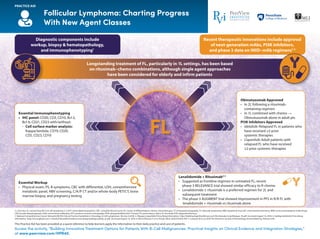
- 1. This Practice Aid has been provided as a quick reference to help learners apply the information to their daily practice and care of patients. 1L: first-line; 2L: second-line; Bcl-2: B-cell lymphoma 2; C/A/P: chest/abdominal/pelvic; CBC: complete blood count; CD: cluster of differentiation; chemo: chemotherapy; CT: computed tomography; FL: follicular lymphoma; HBV: hepatitis B virus; IHC: immunohistochemistry; IMiD: immunomodulatory imide drugs; LDH: lactate dehydrogenase; mAb: monoclonal antibodies; PET: positron emission tomography; PI3K: phosphatidylinositol-3 kinase; PS: performance status; R: rituximab; R/R: relapsed/refractory. 1. National Comprehensive Cancer Network (NCCN) Clinical Practice Guidelines in Oncology. B-Cell Lymphomas. Version 4.2018. 2. Aliqopa (copanlisib) Prescribing Information. http://labeling.bayerhealthcare.com/html/products/pi/Aliqopa_PI.pdf. Accessed August 14, 2018. 3. Zydelig (idelalisib) Prescribing Information. http://www.gilead.com/~/media/Files/pdfs/medicines/oncology/zydelig/zydelig_pi.pdf. Accessed August 14, 2018. 4. Morschhauser F et al. N Engl J Med. 2018;379:934-947. 5. Leonard JP et al. 2018 The American Society of Hematology Annual Meeting. Abstract 445. Access the activity, “Building Innovative Treatment Options for Patients With B-Cell Malignancies: Practical Insights on Clinical Evidence and Integration Strategies,” at www.peerview.com/HPR40. PRACTICE AID Follicular Lymphoma: Charting Progress With New Agent Classes Diagnostic components include workup, biopsy & hematopathology, and immunophenotyping1 Essential Immunophenotyping • IHC panel: CD20, CD3, CD10, Bcl-2, Bcl-6, CD21, CD23 with/without: - Cell surface marker analysis: Kappa/lambda, CD19, CD20, CD5, CD23, CD10 Essential Workup • Physical exam, PS, B symptoms, CBC with differential, LDH, comprehensive metabolic panel, HBV screening, C/A/P CT and/or whole-body PET/CT, bone marrow biopsy, and pregnancy testing Lenalidomide + Rituximab4-5 • Suggested as frontline regimen in untreated FL; recent phase 3 RELEVANCE trial showed similar efficacy to R-chemo • Lenalidomide ± rituximab is a preferred regimen for 2L and subsequent treatment • The phase 3 AUGMENT trial showed improvement in PFS in R/R FL with lenalidomide + rituximab vs rituximab alone Obinutuzumab Approved • In 2L following a rituximab- containing regimen • In 1L combined with chemo → Obinutuzumab alone in adult pts PI3K Inhibitors Approved • Idelalisib: Relapsed FL in patients who have received ≥2 prior systemic therapies • Copanlisib: Adult patients with relapsed FL who have received ≥2 prior systemic therapies Longstanding treatment of FL, particularly in 1L settings, has been based on rituximab–chemo combinations, although single agent approaches have been considered for elderly and infirm patients Recent therapeutic innovations include approval of next-generation mAbs, PI3K inhibitors, and phase 3 data on IMiD–mAb regimens1-3 and immunophenotyping and phase 3 data on IMiD–mAb regimens FL
- 2. PRACTICE AID This Practice Aid has been provided as a quick reference to help learners apply the information to their daily practice and care of patients. Chronic Lymphocytic Leukemia: Charting Progress With New Agent Classes 1L: first-line; 2L: second-line; Bcl-2: B-cell lymphoma 2; BTK: Bruton tyrosine kinase; CBC: complete blood count; CD: cluster of differentiation; CLL: chronic lymphocytic leukemia; IHC: immunohistochemistry; mAb: monoclonal antibodies; PS: performance status. 1. National Comprehensive Cancer Network (NCCN) Clinical Practice Guidelines in Oncology. Chronic Lymphocytic Leukemia/Small Lymphocytic Lymphoma. Version 1.2019. 2. Imbruvica (ibrutinib) Prescribing Information. https://www.imbruvica.com/docs/librariesprovider7/ default-document-library/prescribing-information.pdf. Accessed August 14, 2018. 3. Gazyva (obinutuzumab) Prescribing Information. https://www.gene.com/download/pdf/gazyva_prescribing.pdf. Accessed August 14, 2018. 4. Venclexta (venetoclax) Prescribing Information. https://www.rxabbvie.com/pdf/venclexta.pdf. Accessed August 14, 2018. 5. https://clinicaltrials.gov/ct2/show/NCT02048813. Accessed August 21, 2018. 6. https://clinicaltrials.gov/ct2/show/NCT02477696. Accessed August 21, 2018. 7. https://clinicaltrials.gov/ct2/show/ NCT02475681. Accessed August 21, 2018. Access the activity, “Building Innovative Treatment Options for Patients With B-Cell Malignancies: Practical Insights on Clinical Evidence and Integration Strategies,” at www.peerview.com/HPR40. Diagnostic components include workup, biopsy & hematopathology, and immunophenotyping1 Essential Immunophenotyping • IHC panel: CD3, CD5, CD10, CD20, CD23, cyclin D1 with/without: - Cell surface marker analysis: Kappa/lambda, CD19, CD20, CD5, CD23, CD10 Essential Workup • Physical exam including measurement of liver and spleen size, PS, B symptoms, CBC with differential, and comprehensive metabolic panel Bcl-2 Inhibitor Approved • Venetoclax: For patients with ±17p deletion, as detected by an FDA-approved test, who have received ≥1 prior therapy Obinutuzumab Approved • With chlorambucil for previously untreated CLL Ibrutinib Approved • Adult patients with CLL ± 17p deletion • Phase 3 study testing ibrutinib combinations in 1L CLL (E1912)5 Acalabrutinib6,7 • In phase 3 testing (ELEVATE CLL trials in 1L and 2L settings) • Recommended (NCCN 2018) for relapsed/refractory CLL in frail older pts (≥65 years) and younger patients (<65 years) Historically, treatment of symptomatic CLL was chemotherapy or immunochemotherapy based; in the past several years, novel agent classes have emerged and established roles as part of CLL care Recent therapeutic innovations include approval of next-generation mAbs, BTK inhibitors, and Bcl-2 inhibitors1-4 CLL
- 3. PRACTICE AID This Practice Aid has been provided as a quick reference to help learners apply the information to their daily practice and care of patients. 1L: first-line; 2L: second-line; BR: bendamustine and rituximab; BTK: Bruton tyrosine kinase; C/A/P: chest/abdominal/pelvic; CBC: complete blood count; CD: cluster of differentiation; chemo: chemotherapy; CT: computed tomography; ECG: electrocardiogram; HBV: hepatitis B virus; IHC: immunohistochemistry; IMiD: immunomodulatory drug; LDH: lactose dehydrogenase; MCL: mantle cell lymphoma; MUGA: multiple-gated acquisition; PET: positron emission tomography; PS: performance status; RT: radiation therapy; tx: treatment. 1. National Comprehensive Cancer Network (NCCN) Clinical Practice Guidelines in Oncology. B-Cell Lymphomas. Version 4.2018. 2. Calquence (acalabrutinib) Prescribing Information. https://www.azpicentral.com/calquence/calquence.pdf#page=1. Accessed August 14, 2018. 3. Revlimid (lenalidomide) Prescribing Information. http://media.celgene.com/content/uploads/revlimid-pi.pdf. Accessed August 14, 2018. 4. https://clinicaltrials.gov/ct2/show/NCT03112174. Accessed August 21, 2018. 5. https://clinicaltrials.gov/ct2/show/NCT02972840. Accessed August 21, 2018. Access the activity, “Building Innovative Treatment Options for Patients With B-Cell Malignancies: Practical Insights on Clinical Evidence and Integration Strategies,” at www.peerview.com/HPR40. Mantle Cell Lymphoma: Charting Progress With New Agent Classes Diagnostic components include workup, biopsy & hematopathology, and immunophenotyping1 Essential Immunophenotyping • IHC panel: CD20, CD3, CD5, cyclin D1, CD10, CD21, CD23, Bcl-2, Bcl-6, Ki-67 with/without: - Cell surface marker analysis: Kappa/lambda, CD19, CD20, CD5, CD23, CD10 Essential Workup • Physical exam, PS, B symptoms, CBC with differential, comprehensive metabolic panel, LDH, bone marrow biopsy ± aspirate, C/A/P CT and/or whole-body PET/CT, HBV screening (if rituximab contemplated), ECG or MUGA scan (if anthracycline- or anthracenedione-based regimen is indicated), and pregnancy testing (if chemo or RT planned) IMiD Approved • Lenalidomide: Relapsed MCL in patients who have received ≥2 prior systemic therapies, one of which included bortezomib BTK Inhibitors Approved • Ibrutinib: Adult patients with relapsed MCL who have received ≥2 prior systemic therapies • Ibrutinib–venetoclax combination is being studied in the phase 3 SIMPATICO trial4 • Acalabrutinib: Adult patients with relapsed MCL who have received ≥1 prior therapy • Phase 3 study of 1L acalabrutinib + BR is underway5 Immunochemotherapy, often aggressive in nature, is a mainstay of 1L therapy in MCL; however, relapsed MCL has historically been characterized by poor response rates and overall survival; newer therapies have emerged in the 2L setting that are more active than traditional tx Recent therapeutic innovations include approval of BTK inhibitors and IMiDs1-3 newer therapies have emerged in the 2L setting that are more active than traditional txnewer therapies have emerged in the 2L setting that are more active than traditional tx MCL
- 4. PRACTICE AID This Practice Aid has been provided as a quick reference to help learners apply the information to their daily practice and care of patients. Diffuse Large B-Cell Lymphoma: Charting Progress With New Agent Classes1 1L: first-line; ASCT: autologous stem cell transplant; Bcl: B-cell lymphoma; BTK: Bruton tyrosine kinase; C/A/P: chest/abdominal/pelvic; CAR-T: chimeric antigen receptor T (cell); CBC: complete blood count; CD: cluster of differentiation; chemo: chemotherapy; DLBCL: diffuse large B-cell lymphoma; GCB: germinal center B-cell; HBV: hepatitis B virus; HDT: high-dose chemotherapy; IHC: immunohistochemistry; IPI: International Prognostic Index; IRF4: interferon regulatory factor 4; LDH: lactose dehydrogenase; LVF: left ventricle function; MUGA: multigated acquisition; MUM1: melanoma associated antigen mutated 1; NCCN: National Comprehensive Cancer Network; PS: performance status; R-CHOP: rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisolone; R-EPOCH: rituximab, etoposide phosphate, prednisone, vincristine, cyclophosphamide, and doxorubicin; R/R: relapsed or refractory; RT: radiation therapy. 1. National Comprehensive Cancer Network (NCCN) Clinical Practice Guidelines in Oncology. B-Cell Lymphomas. Version 4.2018. Access the activity, “Building Innovative Treatment Options for Patients With B-Cell Malignancies: Practical Insights on Clinical Evidence and Integration Strategies,” at www.peerview.com/HPR40. Diagnostic components include workup, biopsy & hematopathology, and immunophenotyping Essential Immunophenotyping • IHC panel: CD20, CD3, CD5, CD10, CD45, Bcl-2, Bcl-6, Ki-67, IRF4/MUM1, MYC - Cell surface marker analysis: Kappa/lambda, CD45, CD3, CD5, CD19, CD10, CD20 Essential Workup • Physical exam, PS, B symptoms, CBC with differential, LDH, comprehensive metabolic panel, uric acid, whole-body PET/CT ± C/A/P CT with contrast of diagnostic quality, bone marrow biopsy, calculation of IPI, HBV testing, echocardiogram or MUGA scan (if anthracycline- or anthracenedione- based regimen indicated), pregnancy testing (if chemo or RT planned) Approved CAR-T Cell Therapies • Axicabtagene ciloleucel: Adults with DLBCL after ≥2 prior systemic therapies • Tisagenlecleucel: Adults with R/R DLBCL after ≥2 prior systemic therapies Induction Therapy (Suggestions as per NCCN) • 1L therapy largely remains R-CHOP • Other 1L therapies are R-CHOP14 and R-EPOCH • Anthracycline-sparing immunochemotherapy for pts with poor LVF • Lenalidomide maintenance in pts 60-80 y of age after R-CHOP • Modified immunochemotherapy also available for frail/elderly patients (>80 y of age) with comorbidities • Adjusted high-risk IPI: HDT + ASCT Second-Line and Subsequent Therapy HDT candidates • Multi-agent chemotherapy ± rituximab Non-HDT candidates • Chemotherapy ± rituximab • Brentuximab vedotin for CD30+ disease • Ibrutinib (non-GCB disease) • Lenalidomide ± rituximab (non-GCB disease) Current guidelines, however, suggest the use of novel therapeutics, including immunomodulating agents and BTK inhibitors; other recent therapeutic innovations include the approval of CAR-T cell therapy for relapsed/refractory DLBCL Rituximab-chemotherapy combination remains the standard of care for previously untreated DLBCL DLBCL