
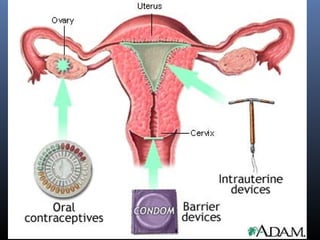



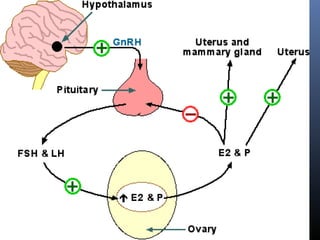
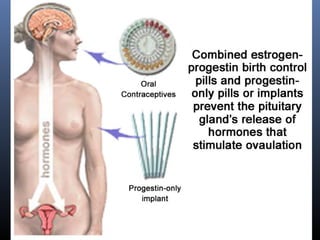



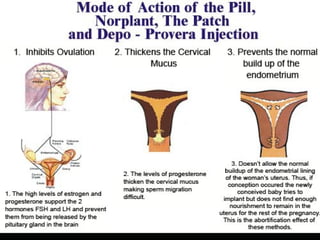














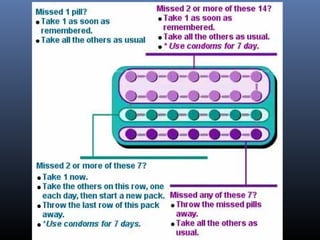


This document discusses hormonal contraceptives, including their mechanisms of action, types, effectiveness, side effects, and considerations for use. It covers oral contraceptives like combined and progestin-only pills, injectables, implants, and emerging options. The main points are: hormonal contraceptives work by suppressing ovulation and thickening cervical mucus; combined oral contraceptives are highly effective but can have side effects; progestin-only options have lower effectiveness and fewer side effects than combined pills; long-acting reversible contraceptives like implants provide years of pregnancy prevention. Risks, drug interactions, and proper use are also outlined.