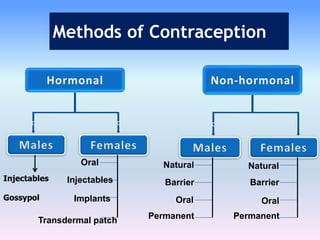
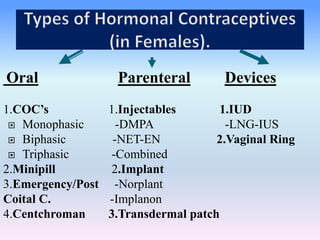
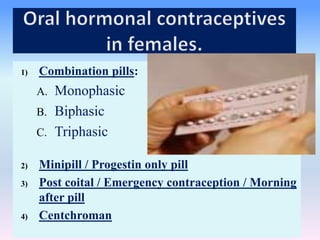
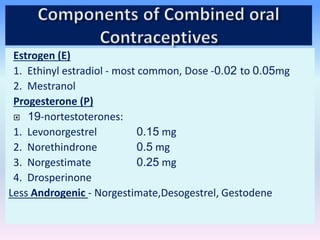
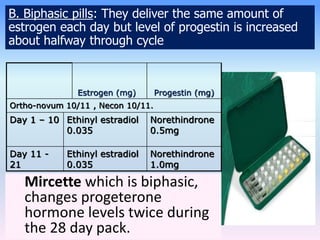
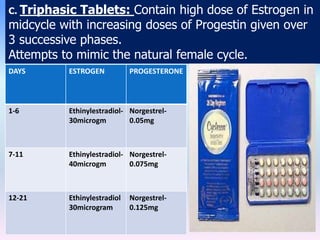
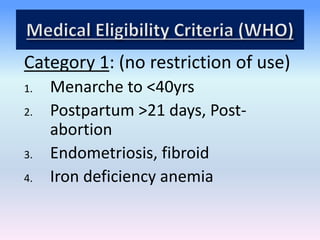
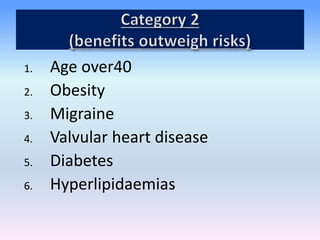
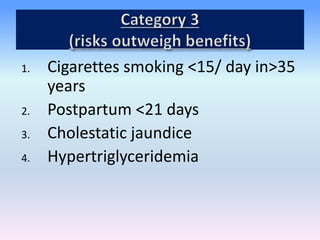
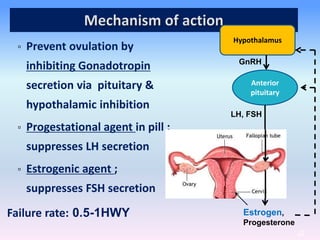
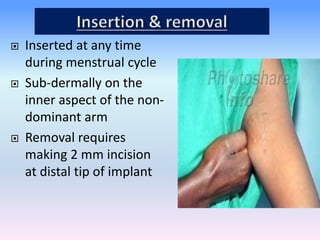
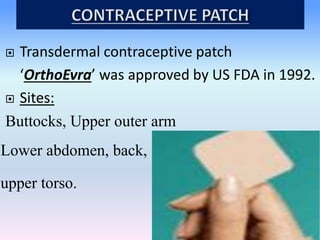
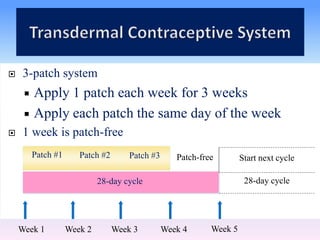
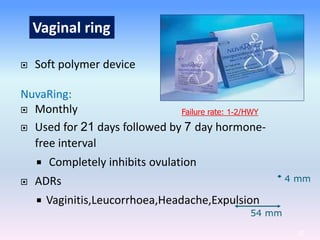
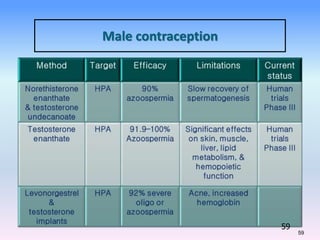
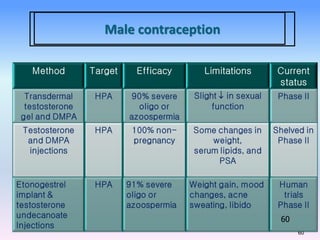
This document discusses various methods of contraception, including natural methods, barrier methods, intrauterine devices, implants, injections, oral contraceptives, and emergency contraception. It provides details on the mechanisms of action, effectiveness, and side effects of different hormonal contraceptives containing progestins and/or estrogens, such as combined oral contraceptives, progestin-only pills, contraceptive patches, vaginal rings, and injectables. The document also discusses criteria for use and cautions for different contraceptive methods.
























































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)


















