Provide education on HIV/AIDS, treatment, self-care, nutrition, stress management, importance of social support, and safe sex practices. Address any psychological issues and provide counseling/referrals as needed.
HISTORY worldwide
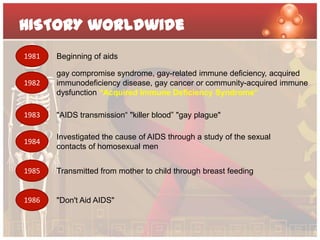
1981 Beginning of aids
gay compromise syndrome, gay-related immune deficiency, acquired
1982 immunodeficiency disease, gay cancer or community-acquired immune
dysfunction “Acquired Immune Deficiency Syndrome”
1983 "AIDS transmission“ "killer blood” "gay plague"
Investigated the cause of AIDS through a study of the sexual
1984
contacts of homosexual men
1985 Transmitted from mother to child through breast feeding
1986 "Don't Aid AIDS"
3.
HISTORY Philippines
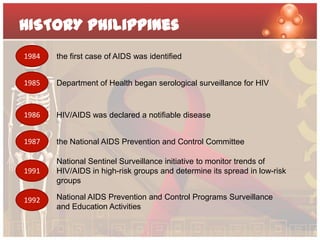
1984 the first case of AIDS was identified
1985 Department of Health began serological surveillance for HIV
1986 HIV/AIDS was declared a notifiable disease
1987 the National AIDS Prevention and Control Committee
National Sentinel Surveillance initiative to monitor trends of
1991 HIV/AIDS in high-risk groups and determine its spread in low-risk
groups
1992 National AIDS Prevention and Control Programs Surveillance
and Education Activities
4.
EPIDIMIOLOGY WORLDWIDE
Number of people Total
33.3 million [31.4 million–35.3
living with HIV Adults
million]
Women 30.8 million [29.2 million–32.6
Children (<15 years)
million]
15.9 million [14.8 million–17.2
million]
People newly Total 2.5 million [1.6 million–3.4 million]
infected Adults
with HIV in 2009 Children (<15 years)
2.6 million [2.3 million–2.8 million]
2.2 million [2.0 million–2.4 million]
AIDS deaths in 2009 Total 370 000 [230 000–510 000]
Adults
Children (<15 years)
1.8 million [1.6 million–2.1 million]
1.6 million [1.4 million–1.8 million]
260 000 [150 000–360 000]
2009
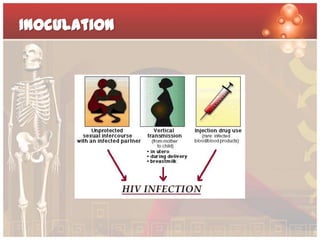
Patient History
• Accordingto the patient’s social and sexual history, he had
been having sex with men he meets at bars. He also had a
live-in partner 2 years ago.
• The client stated that he never had unprotected sex during
sex with men he met at bars.
• The client stated that he was transfused with blood products
after incurring a car accident injury in the past.
9.
Patient History
• Theclient stated that though he takes multivitamins daily and
exercises, even at the gym.
• He said that he does not smoke but drinks occasionally at
least once or twice in a week.
• Lastly, the client stated that he works at a call center agency.
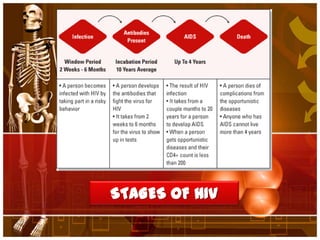
The Stages ofHIV
Infection
• Primary Infection (Acute/ Recent HIV Infection, Acute HIV
Syndrome)
• HIV Asymptomatic (CDC Category A: More than 500 CD4+ T
Lymphocytes/mm3)
• HIV Symptomatic (CDC Category B: 200-499 CD4+ T
Lymphocytes/mm3)
• AIDS (CDC Category C: Fewer than 200 CD4+ T
Lymphocytes/mm3)
13.
Patient symptoms
• Theclient was found to be depressed over the revelation of
his illness, and has not been eating or sleeping well.
• He also stated that even though he easily passed past annual
physical exams, he easily contracts fever and flu.
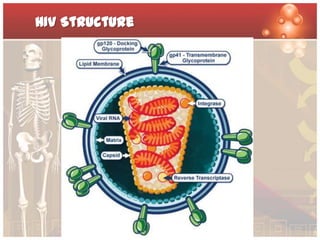
What is HIV?
•Human
Immunodeficiency
Virus, or HIV, is a
sexually transmitted
virus that attacks the
human body’s immune
system.
• Invades helper T-cells/
CD4 cells Via Electron Micrograph by
NIH, 2009
16.
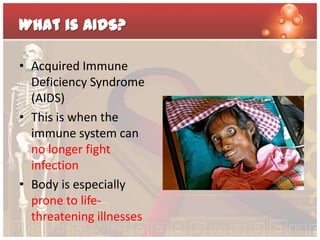
What is AIDS?
•Acquired Immune
Deficiency Syndrome
(AIDS)
• This is when the
immune system can
no longer fight
infection
• Body is especially
prone to life-
threatening illnesses
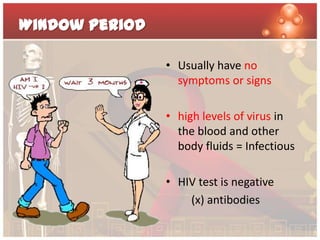
Window Period
• Usually have no
symptoms or signs
• high levels of virus in
the blood and other
body fluids = Infectious
• HIV test is negative
(x) antibodies
20.
Stage 1 (PrimaryHIV Infection or Asymptomatic stage)
• Time Frame: lasts a week or
two
• Often accompanied by a
short flu-like illness
• Production of antibodies
(seroconversion)
21.
Stage 2 (ClinicallyAsymptomatic or Early/ mild stage)
• Time frame: variable;
less than one year to 15
years or more
• 5 to 10% = With health
problems
• Another 5 to 10% =
Asymptomatic
• T-Helper cells =
infected and die
22.
Stage 3 (SymptomaticHIV infection or Intermediate/ Moderate stage)
• Time frame: months to years; 4 or 5 years on average
• immune system becomes increasingly damaged (Mild
symptoms frequent, severe and longer lasting)
• Opportunistic infections/ Cancer
• Multi-system disease
23.
Other symptoms
• Lack of energy
• Weight loss
• Frequent fevers and sweats
• Persistent or frequent yeast infections (oral or
vaginal)
• Persistent skin rashes or flaky skin
• Pelvic inflammatory disease in women that does
not respond to treatment
• Short-term memory loss
• Common symptoms
• Coughing and shortness of breath
• Seizures and lack of coordination
• Difficult or painful swallowing
• Mental symptoms such as confusion and
forgetfulness
• Severe and persistent diarrhea
• Fever
• Vision loss
• Nausea, abdominal cramps, and vomiting
• Weight loss and extreme fatigue
• Severe headaches
24.
Stage 4 (Progressionfrom HIV to AIDS or Late/ Severe AIDS)
• Time frame: Usually less than two years, unless treatment is
available
• CD4 count is less than 200 cells/mm3
• Immune system (very weak) Vulnerability No treatment
DEATH
25.
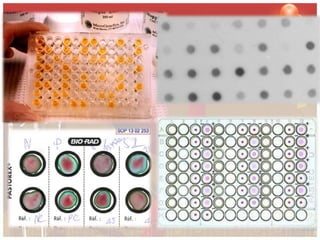
SCREENING tests
3 Types
•ELISA (Enzyme Linked Immunosorbent Assay Test)
• Rapid Tests
Dot Blot
Latex Agglutination Tests
• Simple Test
Particle Agglutination test
Roles of nurses
•Provide health teachings
• Provide information regarding his current medical condition
• Be supportive to the patient and also to his family
• Educate the family or relatives on the proper care of patients
with HIV.
• Trace and screen the client’s past and present partner
34.
Ethical principles
Do no Harm
Autonomy
Equality
Confidentiality
Consent
35.
STIGMA AND DISCRIMINATION
Government
Healthcare
Employment
Restrictions on travel and
stay
Community
Family
36.
PRIORITY NURSING CAREAND TOP
OPPURTUNISTIC INFECTION
Educate the patient of proper hygienic practices to
prevent cross-contamination infection.
Educate the patient of the opportunistic infections and
how to prevent it.
Emphasize the proper ideal lifestyle to reduce further
decrease of the immune system.
GM
Risk for infection related to insufficient knowledge to
avoid exposure to pathogens.
• Note the risk factors for occurrence of infection
• Stress and educate the patient proper handwashing techniques.
• Educate the patient about isolation from others.
• Stress the importance of safe sex practices.
• Review nutritional needs
• Involve the client in community education programs geared to increase
awareness of spread/prevention of communicable diseases
39.
GM
Knowledge deficit regarding the disease process
• Determine client’s ability to learn • Review dietary needs (high protein, High calorie)
and ways to improve intake when depression
• Provide a conducive environment, paced interferes
conversation, allow for feedback
• Stress importance of adequate rest, activity/
• Present information out of sequence, if necessary, exercise
dealing first with the material that is most
anxiety-producing • Trace previous contacts
• Provide positive reinforcement (be more active/ • Know support system of client (family)
excel on work or with family ties than focusing on
risky behavior) • Emphasize compliance with drug regimen
• Instruct patient concerning infection control • Provide information on disease process and future
expectations
• Encourage abstinence or monogamous
relationships and use of latex condoms • Review modes of transmission of disease
• Prescription of anti-retroviral/ anteroviral drugs
40.
GM
Impaired social interaction related to recently
diagnosed medical condition
• Allow patient to verbalize freely his thoughts and perception about his
condition. Be supportive.
• Provide him information regarding his illness.
• Assess his coping mechanisms on his current situation and also his past life
problems.
• Identify availability and stability of support system
• Take note of verbal and nonverbal cues (withdrawal, statements of despair,
sense of aloneness)
• Identify and then refer him to self help groups, community programs
41.
GM
Ineffectivehealth management related to inability make
appropriate judgments
• Asses patient’s knowledge and understanding of condition and treatment
needs
• Determine level of adaptive behavior
• Evaluate environment
• Provide anticipatory guidance
• Encourage socialization
• Provide positive reinforcement
• Provide for communication and coordination
• Promote client participation in planning and evaluation process
Editor's Notes
#3 “Beginning of aids” Around this time a number of theories emerged about the possible cause of these opportunistic infections and cancers. Early theories included infection with cytomegalovirus, the use of amyl nitrite or butyl nitrate 'poppers', and 'immune overload'. Because there was so little known about the transmission of what seemed to be a new disease, there was concern about contagion, and whether the disease could by passed on by people who had no apparent signs or symptoms. Knowledge about the disease was changing so quickly that certain assumptions made at this time were shown to be unfounded just a few months later.
#4 The NAPCC focuses on six activities: surveillance, health education, training of health workers, counseling, screening of blood units and strengthening of diagnostic facilities. This integrated program has identified three long-term goals: to reduce transmission of HIV infection to prevent development of STD complicationsto reduce the impact of HIV infection.56 Issues in Management of STDs in Family Planning SettingsMid-term goals of the program are to:monitor the incidence of infection among identified sentinel groups and the general population continuouslyimplement mandatory HIV screening of all blood productspromote safe sexual behavior, in particular condom usagepromote disinfection practices for skin piercing instrumentspromote health education among individuals at high risk for STDs and HIV/AIDS and among thegeneral populationIntroduction of Genital Tract Infection Services at the Fertility Care CenterFollowing training, genital tract infection services were introduced at the Fertility Care Center (FCC) of the University of the Philippines/Philippine General Hospital and Reproductive Health Care Center. The GTI program has five components:history taking/screening/risk assessmentclinical diagnosislaboratory diagnosistherapeutic management counseling
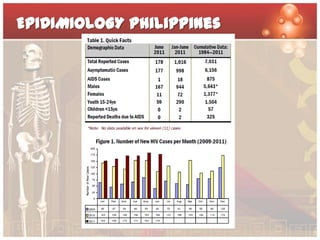
#6 In June 2011, there were 178 new HIV Absero-positive individuals confirmed by the STD/AIDS Cooperative Central Laboratory (SACCL) and reported to the HIV and AIDS Registry (Table 1). This was a 63% increase compared to the same period last year (n=109 in 2010) [Figure 1].Most of the cases (94%) were males. The median age was 28 years (age range:15-58 years). The 20-29 year (60%) age-group had the most number of cases. Sixty-two percent (111) of the reported cases were from the National Capital Region (NCR). Reported mode of transmission was sexual contact (173). Five did not report mode of transmission [Table 2]. Males having sex with other Males (83%) were the predominant type of sexual transmission [Figure 2]. Most (99%) of the cases were still asymptomatic at the time of reporting [Figure 3]. There were no reported deaths for this month.


![EPIDIMIOLOGY WORLDWIDE
Number of people Total
33.3 million [31.4 million–35.3
living with HIV Adults
million]
Women 30.8 million [29.2 million–32.6
Children (<15 years)
million]
15.9 million [14.8 million–17.2
million]
People newly Total 2.5 million [1.6 million–3.4 million]
infected Adults
with HIV in 2009 Children (<15 years)
2.6 million [2.3 million–2.8 million]
2.2 million [2.0 million–2.4 million]
AIDS deaths in 2009 Total 370 000 [230 000–510 000]
Adults
Children (<15 years)
1.8 million [1.6 million–2.1 million]
1.6 million [1.4 million–1.8 million]
260 000 [150 000–360 000]
2009](https://image.slidesharecdn.com/hivfinal-111206095901-phpapp01/85/HIV-case-analysis-4-320.jpg)



















































![Hiv aids part 1[6]](https://cdn.slidesharecdn.com/ss_thumbnails/hivaidspart16-111114103159-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)

































