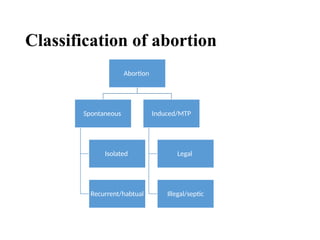
The document discusses abortion, covering definitions, types, causes, management, and Ethiopian abortion law. It defines abortion, classifies various types (e.g., spontaneous, induced, septic), outlines clinical features and management strategies, and provides an overview of the legal framework concerning abortion in Ethiopia, particularly historical changes in law. The document emphasizes the complexities of abortion's medical and legal aspects, including risks, treatments, and evolving legal interpretations over time.

































![ABORTION -POST ABORTIVE CARE[1][2] ner.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/abortion-postabortivecare12ner-250903092827-23f6f291-thumbnail.jpg?width=640&height=640&fit=bounds)














































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)






