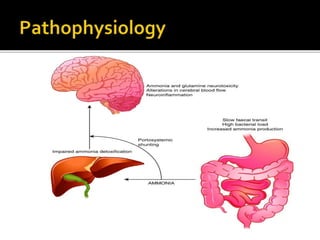
Hepatic encephalopathy is a neuropsychiatric syndrome resulting from acute or chronic liver failure, causing toxins to affect the central nervous system. Symptoms range from confusion to coma, with treatments focusing on identifying and removing precipitating factors, dietary restrictions on protein, and specific medications like lactulose and antibiotics. In severe cases, liver transplantation may be considered for nonresponsive patients.




























![Hepatic encephalopathy [HE]](https://cdn.slidesharecdn.com/ss_thumbnails/hepaticencephalopathy-200612174704-thumbnail.jpg?width=640&height=640&fit=bounds)






































