Downloaded 221 times

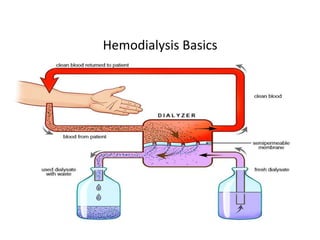


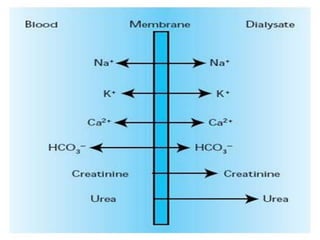







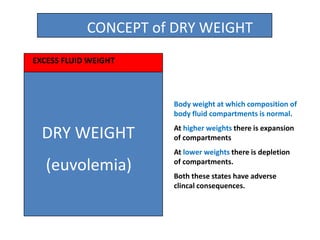
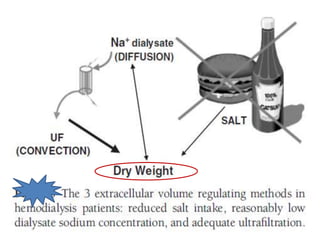






















1. Hemodialysis involves removing fluid and solutes from the body through diffusion and convection to achieve "dry weight." Careful fluid removal is needed to minimize hypotension risks. 2. Blood pressure fluctuates significantly during hemodialysis due to changes in vascular volume, cardiac output, and systemic vascular resistance. Both hypotension and hypertension are common complications. 3. Preventing intradialytic blood pressure issues involves accurate dry weight determination and gradual, steady ultrafiltration. Treatment of issues focuses on fluid balance, vasoactive medications, and optimizing dialysis prescription elements like sodium and temperature.






















































































