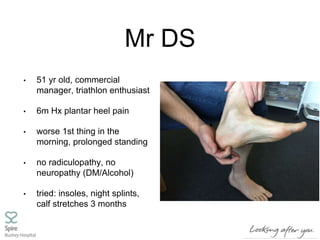
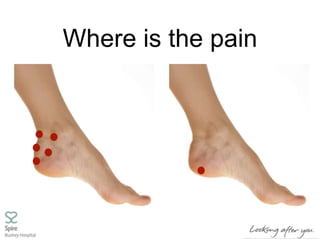
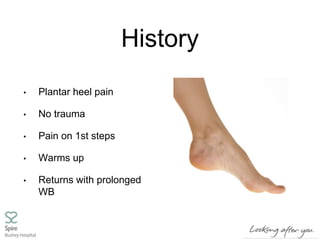
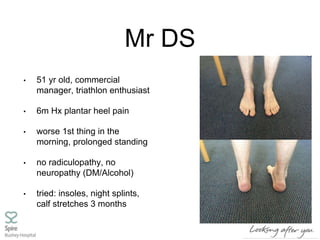
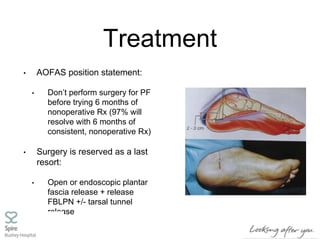
- Mr. DS is a 51-year-old man who experiences plantar heel pain that worsens with prolonged standing and first thing in the morning. He has tried various non-operative treatments for 6 months with limited improvement.
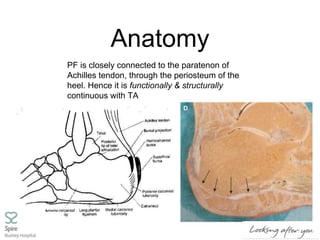
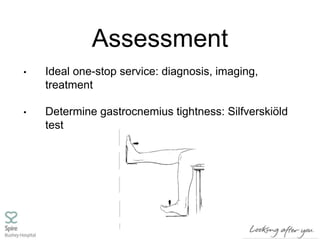
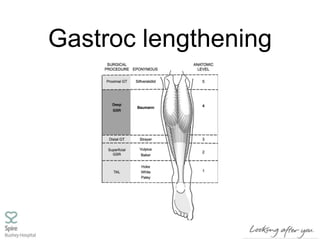
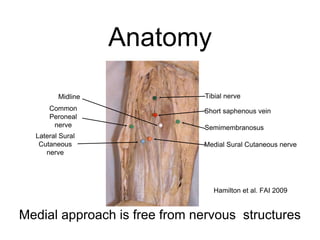
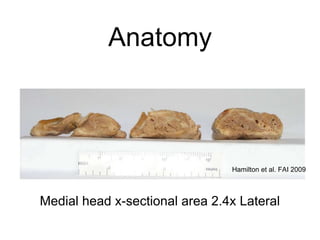
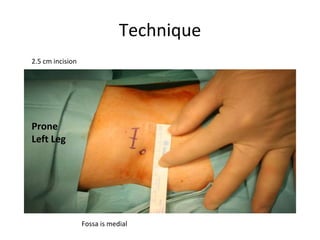
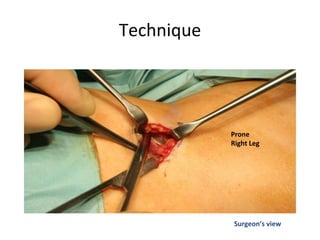
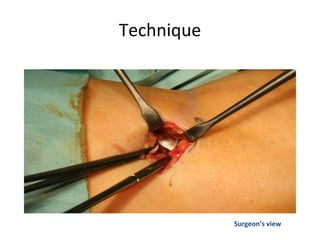
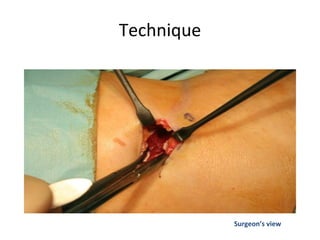
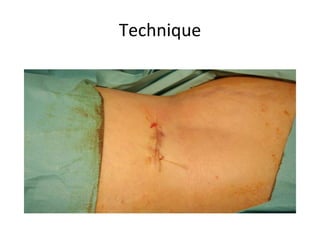
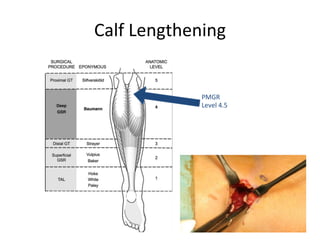
- Gastrocnemius contracture can be associated with plantar heel pain and is assessed using the Silfverskiöld test. Surgical lengthening of the gastrocnemius via the percutaneous medial gastrocnemius recession technique may help recalcitrant plantar fasciitis cases.
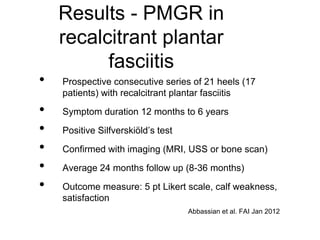
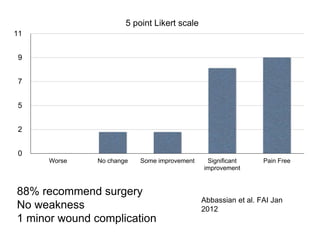
- A prospective study found that 88% of patients reported significant or full improvement after gastrocnemius lengthening surgery for recalcitrant plantar fasciitis, with no