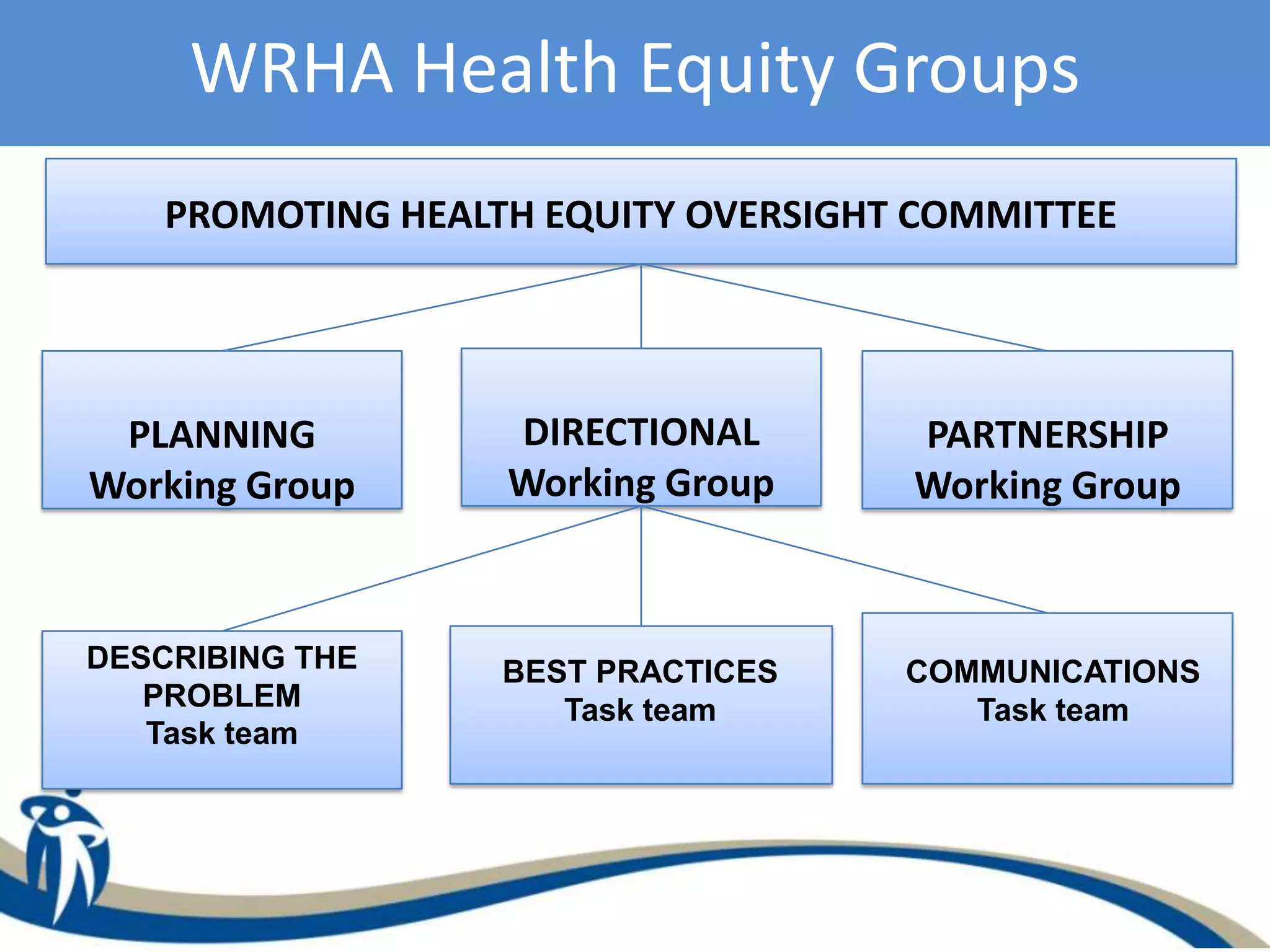
This document describes a case study of efforts in Winnipeg, Canada to increase awareness and action around health equity internally within the Winnipeg Regional Health Authority (WRHA). It outlines challenges faced in developing common ownership of health equity, finding necessary evidence and resources, maintaining leadership motivation, determining roles, establishing priorities, and overcoming competing budgets. Strengths included cross-sector involvement and endorsement from senior WRHA management. Outcomes to date included incorporating health equity into regional planning and strategic public health plans focused on community need.





































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)